
You’ve done everything right.
You went to your primary care doctor. They ran the standard panels, found nothing, and told you to rest. You pushed. Through endless research and self-advocacy, you found a Long COVID clinic – maybe a university program, maybe a telehealth practice, maybe an integrative specialist someone in your online support group recommended. You spent a significant amount of money on testing and extensive protocols, waiting to get better.
You’re still sick.
If that describes your experience, this post is for you. Our goal is to honestly explain something that most Long COVID and Post-Vaccine Syndrome clinicians — even well-meaning, intelligent ones — fundamentally misunderstand about this condition.
At Leading Edge Clinic, we’ve treated more than 3,500 patients with Long COVID and Post-Vaccine Syndrome. Many of them came to us after failing at other practices, sometimes after spending $30,000 to $100,000 elsewhere. What we’ve observed over years of clinical work has shaped a different understanding of why standard approaches so often fall short.
The Core Problem: Long COVID Is Not One Disease
The most common clinical mistake we see, across conventional medicine, integrative medicine, and Long COVID specialty practices alike, is treating this condition as if it has a singular mechanism that responds to a singular approach (ie: dealing only with spike persistence, dealing only with immune dysfunction, looking only at gut health, etc…)
It doesn’t.
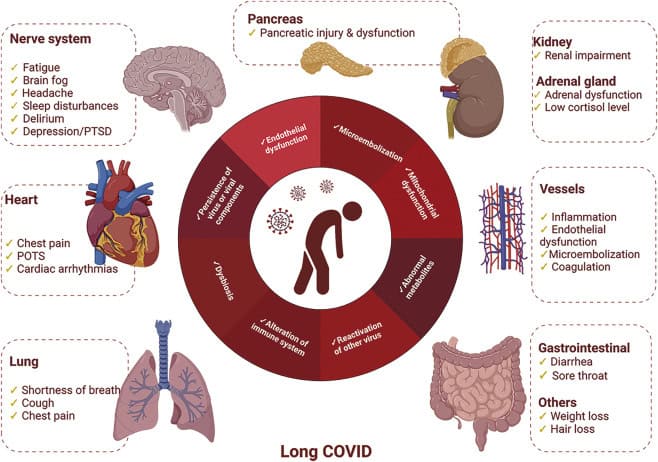
Long COVID and Post-Vaccine Syndrome are multi-system, multi-mechanism conditions that present differently in every patient and evolve over time. What’s driving your fatigue may not be the same as what’s driving the next patient’s. And critically, what’s driving your symptoms today may not be what’s driving them six months from now.
Like other historicaly post-viral and post-vaccine syndromes, this not a simple infection with a clean recovery arc. It is a dysregulated biological state, and it is very effcient at driving that dysregulated state — often involving the immune system, the nervous system, the vascular system, and the metabolic system simultaneously, in proportions that vary person to person and shift in response to treatment.
A clinician who approaches it with a fixed protocol, even a sophisticated one, is going to miss the mark for a significant portion of patients.
What Standard Approaches Miss
This is not an exhaustive list. It hits on some major systemic issues we don’t see others talking about, but these aren’t the only things we see other clinicians missing when a new patient comes to us that has tried elsewhere first.
1. They Don’t Account for Cell Danger Response
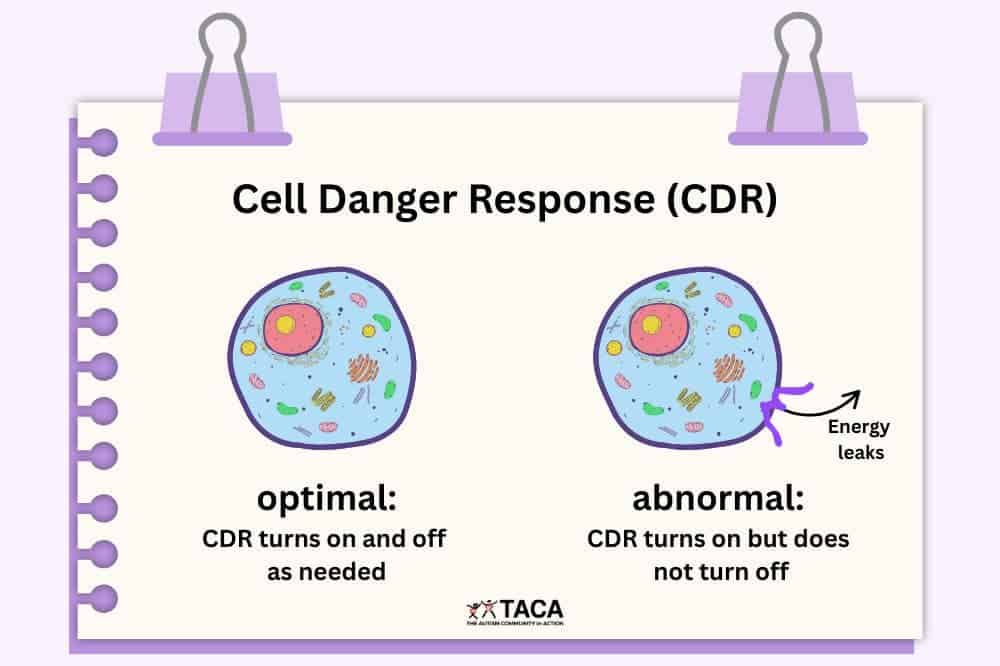
One of the most underappreciated mechanisms in Long COVID is something called the Cell Danger Response (CDR) — a concept developed by metabolic researcher Dr. Robert Naviaux.
The CDR is the body’s ancient, conserved response to threat. When cells detect danger, such as infection, toxin, or injury, they shift into a defensive metabolic state. Energy production is reduced, cellular communication slows down , and cells essentially go quiet to protect themselves.
This is adaptive in the short term. After an acute COVID infection, you want this response. It’s doing its job.
The problem is when the CDR doesn’t turn off. When the body’s threat detection system remains activated long after the initial danger has passed, you get persistent metabolic suppression. This manifests as fatigue that doesn’t resolve with rest, cognitive dysfunction that doesn’t respond to sleep, and a nervous system that stays in a low-grade defensive posture.
Most Long COVID clinicians are not testing for or thinking about CDR biology. Many deal with chronic inflammation and persistent spike protein, but never take that next step to address chronic CDR.
2. They Don’t Understand Senescent Cells
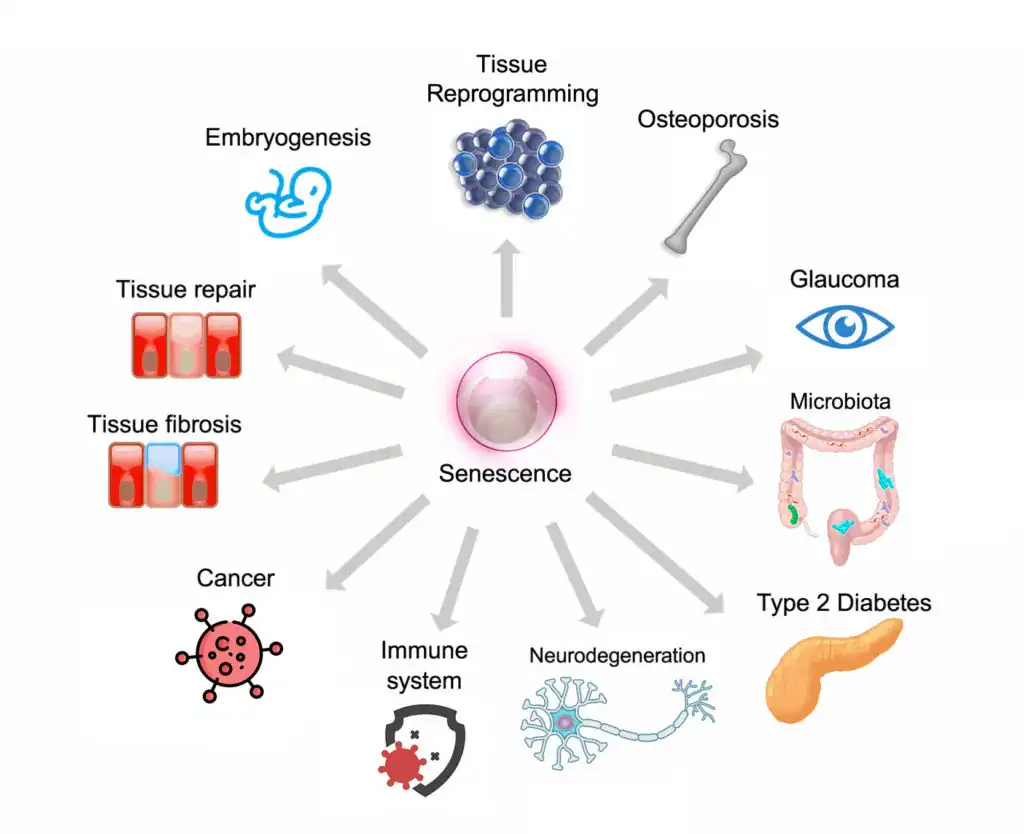
Cellular senescence, what some researchers call the “zombie cell” problem, is another mechanism that rarely appears in standard Long COVID treatment frameworks, although it may accidentally be addressed (albeit not thoroughly enough) through treatments with other prescribed purposes.
Senescent cells are cells that have stopped dividing but refuse to die. In the aftermath of a severe immune activation like COVID infection, the body can accumulate these cells in significant numbers. In fact, the spike protein seems to have be very skilled at producing senescent cells. These cells don’t do their normal jobs, but they also release a continuous stream of pro-inflammatory signaling molecules, the senescence-associated secretory phenotype (or SASP).
The result of senescent cell accumulation is a low-grade, chronic inflammatory state that can persist for years. Standard anti-inflammatory approaches don’t clear senescent cells. Senolytics, which are treatments that induce apoptosis in senescent cells, are rarely considered in clinical practice, let alone in Long COVID or Post-Vaccine Syndrome.
For patients where senescent cell burden is a significant contributor, which is all spike protein patients, treating everything else while ignoring this mechanism is like bailing water from a boat without fixing the leak.
3. They Apply Uniform Protocols to Non-Uniform Patients
We understand why this happens. Protocols are efficient. They can be standardized, taught, and scaled. If you’re running a practice that sees 50 Long COVID patients a week, a decision tree makes sense. Our practice model focuses on lower patient volumes for more personalized care and treatment. Why?
Long COVID patients are not uniform. The neurotransmitter profile of one patient – the specific pattern of catecholamine deficiency, glutamate dysregulation, and kynurenine pathway disruption – may look nothing like the next patient’s. The autoimmune burden, the degree of microclotting, the level of residual spike protein activity, the autonomic dysfunction pattern, may all vary enormously from patient to patient.
Our practice partner Scott Marsland, FNP-C, published a detailed case study that illustrates this complexity in just one patient, examining neurotransmitter changes across time and in response to specific interventions. The data showed 13 of 27 measured neurotransmitters were outside optimal range at baseline. The specific pattern of elevated glutamate suggesting excitotoxicity, paradoxically elevated serotonin alongside low tryptophan, and depleted catecholamines required a tailored response, not a standard protocol. And the picture changed meaningfully over seven months, requiring ongoing adjustment.
That is what individualized Long COVID care actually looks like.
4. They Over-Test and Under-Treat
There are particular kind of specialty practices that run $2,000–$5,000 in laboratory panels before doing much of anything. The testing is framed as “comprehensive” and “data-driven.” It feels thorough. As humans, we want to latch onto something concrete, like lab results. It gives us something to work at, and improve upon.
But here’s the honest clinical reality: in most Long COVID and PACVS patients, extensive testing rarely changes the initial treatment approach. The patterns we see across 3,500+ cases are recognizable. The likely mechanisms become apparent through careful history, symptom characterization, and clinical pattern recognition long before any lab results return.
Excessive testing delays treatment. It costs patients money they could have spent on interventions. And it creates an illusion of certainty in a condition that requires the intellectual honesty to acknowledge: we are treating this by thoughtful trial, observation, and adjustment. Running a panel and following a chart does not work for complex conditions like Long Covid and Post-Vaccine Syndrome. One day might turn up a normal lab result, and then many abnormalities the next testing period. Patients end up chasing ghosts.
And, by the way, if and when a $4,000 testing panel arrives that meaningfully guides pin-pointed treatment decisions tha deliver results, we will be the first ones to come back and edit this post.
5. They Treat the First Layer and Stop
Long COVID recovery, when it happens, typically unfolds across 9 to 18 months. Sometimes longer. The condition does not resolve in a single treatment arc, but requires ongoing attention to how the patient’s picture is shifting.
A treatment that was appropriate in month two may need modification by month five. An intervention that wasn’t relevant initially may become important as other issues resolve and different mechanisms become more apparent. The clinical work is iterative.
Many practices, particularly those operating at high volume or on a brief-consultation model, don’t have the infrastructure or clinical philosophy to support this. They prescribe an initial regimen and check in only when you schedule your next appointment. That interval is too long, and the flexibility to pivot is often not there.
What a Different Approach Looks Like
We want to be direct about what we actually do differently, not just what we criticize.
We start with clinical reasoning, not a panel. The first consultation at Leading Edge Clinic is 60 minutes. We are building a detailed picture of your symptom history, your illness trajectory, what you’ve tried, how you responded, and what the pattern suggests. That reasoning guides our initial approach, not a lab panel.
We think about mechanisms, not just symptoms. If you have fatigue, we want to understand whether it’s primarily metabolic, autonomic, inflammatory, or driven by a cellular danger response that hasn’t resolved. Different mechanisms call for different interventions.
We are honest about the trial-and-error nature of treatment. We don’t tell patients we’ve found the answer and here it is. We tell them: here is our best clinical hypothesis, here is the treatment we think is most likely to move things in the right direction, and here is how we’ll know if it’s working. We adjust based on what we observe.
We treat the evolving patient, not the initial presentation. Follow-up is built into how we work. As patients respond, we incorporate that information and adapt.
We consider mechanisms that others don’t. Cell danger response, cellular senescence, persistent spike protein activity, microclotting, neurological changes, autonomic dysfunction, immune dysregulation, MCAS, and other spike protein pathologies are all part of our clinical thinking. Not for every patient, but for the patients where these mechanisms are relevant, addressing them can be the difference between continued decline and meaningful recovery.
What You Should Ask Any Long COVID Specialist
If you’re evaluating whether a Long COVID practice is right for you, here are honest questions worth asking:
“What do you think is driving my specific symptoms?” A clinician who can give you a mechanistic hypothesis, specific to your history, and not a generic answer, is thinking carefully. A clinician who gives you the same answer they give everyone is running a protocol.
“What do you do when a treatment isn’t working?” The answer should involve active pivoting, consideration of alternative mechanisms, and willingness to try something different.
“How do you think about conditions like cell danger response or cellular senescence?” You’re not expecting a dissertation. But a blank look or a dismissive response tells you something about the depth of the clinical framework.
“How long do you expect treatment to take?” Honesty here matters. Anyone promising significant recovery in 6 to 8 weeks is either treating very mild cases or not being straight with you. The realistic timeline for meaningful improvement in complex Long COVID is 9 to 18 months.
A Note on What We Don’t Promise
We’ve seen enough patients and enough trajectories to say this plainly: approximately 80–85% of our patients achieve significant functional improvement over the course of treatment. That is a meaningful number, and we’re proud of it.
But 80–85% also means that 15–20% of patients don’t reach that threshold, at least not within our treatment window.
What we can promise is clinical honesty, genuine intellectual engagement with your case, and a willingness to keep thinking when the obvious approaches aren’t working.
If You’ve Already Tried Everything
If you’ve been through the conventional system, the university Long COVID clinics, the integrative medicine practices, the telehealth protocols – and you’re still significantly impaired – there may be value in a clinical framework that explicitly accounts for the mechanisms most others aren’t addressing.
We recognize that many of our patients come to us precisely because they’ve exhausted the obvious options and need something different.
A 60-minute initial evaluation gives us the opportunity to build a complete picture of your case: what you’ve tried, how you responded, what your symptom pattern suggests, and where we think there may be unexplored mechanistic territory. From that, we develop a realistic treatment roadmap, not a protocol applied to a category, but a clinical plan developed for your specific situation.
You can register as a patient here.
The Bottom Line
Long COVID and Post-Vaccine Syndrome not one disease. They don’t have one mechanism, they don’t respond to one protocol, and they don’t resolve on a predictable timeline.
The clinicians who are having the best outcomes with this condition are the ones who understand complexity, think in terms of mechanisms, are willing to adapt, and have the clinical experience to recognize patterns that don’t fit neatly into any category.
That is the medicine we practice. If you’ve been failed by other approaches and you’re still looking for meaningful progress, we’d be glad to talk.
Leading Edge Clinic specializes in Long COVID, Post-Vaccine Syndrome, and complex post-infectious illness. Our clinic has treated more than 3,500 patients with these conditions.
This article is for informational purposes and does not constitute medical advice. Individual results vary.