
Introduction: The Crash That Doesn’t Make Sense
A walk around the block, a few hours of focused work, a social event, or a workout you thought you were finally ready for. It didn’t feel excessive at the time.
Then, 12 to 72 hours later, something happened that has no parallel in “normal” human experience. Not tiredness. Not soreness. A complete systemic collapse, with fatigue so profound it feels neurological, brain fog that makes thinking feel like wading through quicksand, muscle pain, sensory sensitivity, and a return of every symptom you thought you’d been making progress on.
This is post-exertional malaise. And if you have Long COVID or Post-Vaccine Syndrome, you’ve almost certainly experienced it.
What you may not have received is an honest clinical explanation of what it actually is, why it happens, and why the treatment most clinicians prescribe — pushing through, gradually increasing activity, “deconditioning” management — is not just ineffective but genuinely harmful.
At Leading Edge Clinic, we treat PEM as one of the most mechanistically complex and most clinically important features of Long COVID and Post-Vaccine Syndrome. Getting it wrong doesn’t just stall recovery. It actively damages the biology you’re trying to repair.
What Post-Exertional Malaise Actually Is
PEM is formally defined as the worsening of symptoms following physical, mental, or cognitive exertion. It typically occurs with a delay of 12 to 48 hours after the triggering activity, and can last days to weeks.
The delay is important because it’s what makes PEM so consistently misunderstood by clinicians who aren’t familiar with it. If you crashed immediately after exertion, it would feel like an obvious cause-and-effect relationship. The delay means that by the time you feel the worst of it, you’ve already returned to baseline and the connection to what you did two days ago is no longer obvious. Patients are told their symptoms are unrelated to exercise. Sometimes they get an even worse explanation… “it’s all in your head”. Clinicians interpret the crash as a separate event rather than a predictable physiological consequence.
PEM is not deconditioning. It is not anxiety. It is definitely not a failure of effort or will – many of our patients were often “high achievers” prior to their illness. PEM is a specific, reproducible, biologically mediated response to exertion that occurs in a body with compromised cellular energy production, impaired microcirculation, and immune dysregulation. Even the mainstream research now makes this unambiguous.
The Biology: What Is Actually Happening During a PEM Crash
Mitochondrial Dysfunction at the Core
The most important mechanistic development in understanding PEM in Long COVID came from a series of muscle biopsy studies — most notably the 2024 landmark study published in Nature Communications by Appelman, Charlton, and colleagues at Amsterdam UMC, and the accompanying opinion article in Trends in Endocrinology and Metabolism by the same group.
What these studies found in the skeletal muscle tissue of Long COVID patients was as follows: intrinsic mitochondrial dysfunction, not just as a baseline impairment, but one that worsened measurably after exercise. Mitochondrial respiration (the process by which cells produce ATP) decreased significantly one day after maximal, PEM-inducing exercise. Markers of mitochondrial density dropped. The muscle showed acute tissue damage, focal necrosis, and intramuscular infiltration of immune cells that was not present before the exercise challenge.
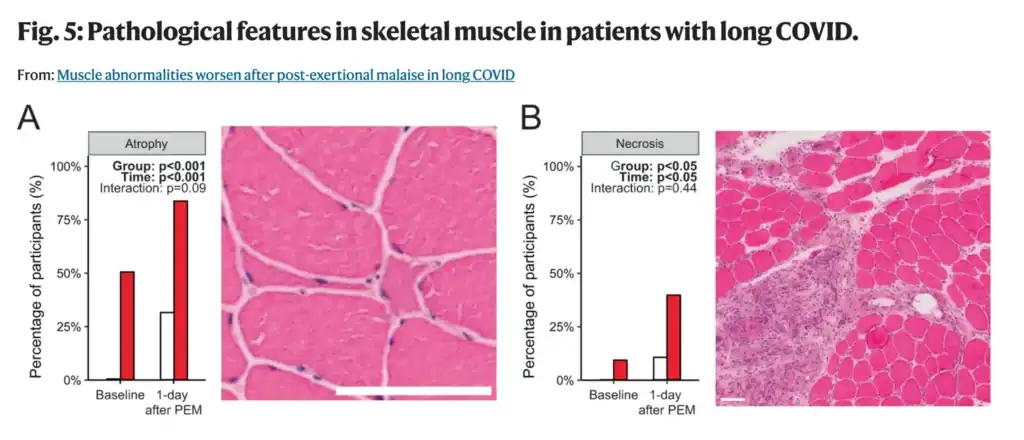
This is not deconditioning. A deconditioned person’s muscles don’t necrotize after moderate exercise. What’s happening in Long COVID and Post-Vaccine Syndrome PEM is closer to a pathological injury response. The tissue cannot meet the energetic demand placed on it, and the attempt to do so causes measurable cellular damage.
The same research group also identified a shift in muscle fiber type, away from slow-twitch oxidative fibers and toward fast-twitch glycolytic fibers. This matters because oxidative fibers rely on efficient mitochondrial energy production for sustained activity. Glycolytic fibers burn energy quickly but produce lactate rather than sustained ATP. We have heard countless times from patients describing their PEM, some variation of, “it feels like my entire body is full of lactic acid. Like I’ve been poisoned.” A muscle that has shifted toward glycolytic metabolism will hit an energy wall faster, recover more slowly, and be more vulnerable to the kind of anaerobic overload that characterizes PEM.
The Microcirculation Problem
The mitochondrial dysfunction doesn’t occur in isolation. It is compounded by, and in part caused by, the endothelial dysfunction and microclotting that are central features of Long COVID.
When capillary beds are partially obstructed by amyloid fibrin microclots, oxygen delivery to working muscle tissue is impaired. The mitochondria of a Long COVID patient’s muscle cells may be operating in a relative hypoxic environment, even at rest. Under the increased oxygen demand of exercise, that deficit becomes significant. The tissue is asked to produce more energy precisely when its oxygen supply is most constrained.
A 2023 study in Acta Neuropathologica confirmed that Long COVID patients show capillary alterations and immune dysregulation in skeletal muscles. In other words, the physical infrastructure of oxygen delivery to muscle tissue is damaged. You cannot exercise your way out of damaged capillaries. Graded exercise therapy aimed at improving mitochondrial function in these patients is asking an engine with a clogged fuel line to run harder.
The Immune Activation Component
Exercise, even moderate exercise, triggers an inflammatory response in healthy individuals. The muscles release cytokines. Immune cells infiltrate tissue. This is part of normal adaptation and recovery. In healthy individuals, the process resolves and the tissue rebuilds stronger.
In Long COVID and Post-Vaccine Syndrome patients with already-elevated inflammatory signaling (already-elevated IL-6, already-activated mast cells, already-dysregulated immune responses), exercise delivers an additional inflammatory load onto a system with no reserve capacity to manage it. The immune activation triggered by exercise doesn’t resolve normally. It compounds the existing inflammatory state, triggering the systemic symptom cascade that characterizes a PEM crash.
Research published in PMC in 2025 confirmed that PEM in Long COVID is mediated by dysfunctions in both mitochondrial capacity and microcirculation, maintained by latent immune activation that conjointly impairs peripheral bioenergetics. This is not a psychological phenomenon. It is a coordinated biological failure at the cellular and vascular level.
The Cell Danger Response Connection
There is a deeper layer to PEM that connects to the Cell Danger Response framework we’ve written about previously.
When cells are in an active CDR state (as many Long COVID and Post-Vaccine Syndrome patients’ cells are), exertion represents exactly the kind of additional stressor that further activates the danger signaling cascade. ATP is released into the extracellular space as a danger signal. The purinergic signaling system, already dysregulated, interprets the metabolic stress of exercise as renewed threat. Rather than recovering normally, cells double down on the defensive metabolic state, suppressing normal energy production further, perpetuating the CDR, and deepening the very dysfunction that made exercise difficult in the first place.
This mechanism helps explain why PEM can leave patients worse off than before the triggering activity, not just temporarily, but potentially persistently if the CDR activation is severe enough to push cells further into the senescent cascade.

The Graded Exercise Therapy Problem
Here is the clinical position that many uninformed clinicians are still operating from: Long COVID fatigue and exercise intolerance are primarily driven by deconditioning, and the solution is gradual, progressive increases in physical activity. This is also known as Graded exercise therapy, or GET.
This position is not just wrong, it is dangerous. It has been formally disputed by clinicians and researchers on the basis of the biological evidence, it was used in the ME/CFS context based on a deeply flawed trial (the PACE trial), and its application to Long COVID (and PACVS) patients with PEM has been specifically and publicly opposed by leading researchers including those at Amsterdam UMC, Mt. Sinai, and multiple European academic centers.
In January 2024, a letter published in Nature signed by Dutch, German, and Austrian investigators (joined by David Putrino of Mt. Sinai) stated explicitly: “We cannot agree with the recommendations for graded exercise therapy for people living with Long COVID who have post-exertional malaise.” The letter noted that the PACE trial, which is frequently cited in support of GET, has had its results called into question due to substantial protocol deviations and retrospective adjustment of recovery criteria. Improperly interpreted and manipulated study design and results? Where else have we seen that?
Professor Todd Davenport, a physical therapy researcher at the University of the Pacific, stated bluntly in 2024: “Any article published in 2024 citing the PACE trial as evidence of safety and efficacy of graded exercise should not be taken seriously.”
A review of exercise trials in Long COVID published in The Sick Times in late 2025 found that of 112 exercise-related trial registrations for Long COVID, fewer than 20% even mentioned PEM. Of those that did, two excluded participants with moderate-to-severe PEM and two excluded PEM participants entirely. The research community is studying exercise in Long COVID while systematically excluding the patients for whom exercise is most dangerous.
The deconditioning model fails for a simple reason: a deconditioned person’s skeletal muscle does not show focal necrosis, mitochondrial enzyme collapse, and immune cell infiltration after moderate exercise. That is what Long COVID patients’ muscle tissue shows. The biology is not consistent with deconditioning. It is consistent with a pathological injury response in tissue that lacks the cellular and vascular infrastructure to handle exertional demand.
What Appropriate PEM Management Actually Looks Like
If graded exercise therapy is the wrong answer, what is the right one? The honest clinical answer has two parts: understanding your energy envelope, and treating the underlying mechanisms that are causing PEM in the first place.
Pacing and the Energy Envelope
Pacing is not giving up. Many patients struggle to reconcile between their former selves, and their new physical constraints. But, pacing is a clinically rational strategy based on the biology of PEM. Specifically, the observation that there is a physiological threshold below which activity is tolerable and above which it triggers the pathological crash cascade.
The goal of pacing is to identify and stay within your energy envelope. Your energy envelope is the level of exertion your body can sustain without triggering post-exertional symptom worsening. This requires honest, often uncomfortable acceptance that your current energy envelope may be far smaller than your pre-illness capacity. Attempting to expand that envelope by pushing through symptoms (the instinct that works for normal fatigue, and has been socially built into many of our mindsets) actively damages the biology you’re trying to repair. It is easy to understand why patients may feel like they are going to “fall behind”, when adapting to this newfound situation.
Heart rate monitoring can be a useful pacing tool. Research suggests that staying below the anaerobic threshold, often approximated as 50–60% of age-predicted maximum heart rate in Long COVID patients, reduces the probability of triggering a crash. This is a lower threshold than most patients expect and lower than most clinicians prescribe.
Another extremely important and nuanced note… Cognitive and emotional exertion count. PEM is not exclusively triggered by physical activity. Mental effort, social interaction, sensory stimulation, and emotional stress can all trigger crashes in patients with significant PEM. This is consistent with: 1) the neurological and circulating contributors to PEM that the research has identified; and 2) the physiological facts that our brains account for 20% of our daily energy expenditure. All this means that pacing must encompass the full scope of daily exertion, not just physical exercise.

Treating the Underlying Mechanisms
Pacing manages the symptom. It does not treat the cause. For Long COVID and Post-Vaccine Syndrome patients, the cause of PEM is the biological substrate described above: mitochondrial dysfunction, impaired microcirculation, immune dysregulation, and the ongoing CDR state and senescent cell burden.
Addressing microclotting. If capillary obstruction from amyloid fibrin microclots is impeding oxygen delivery to muscle tissue, reducing that obstruction through appropriate fibrinolytic support guided by clinical assessment (and where relevant, PAI-1 genotype) directly addresses one of the key contributors to PEM.
Mitochondrial support. The evidence for mitochondrial dysfunction in PEM is now well-established. Supporting mitochondrial function represents a rational clinical approach, though responses are individual and should be guided by a clinician familiar with this patient population.
Reducing the inflammatory environment. Since immune activation during exercise compounds the existing inflammatory state and drives PEM crashes, reducing the baseline inflammatory burden expands the effective energy envelope over time.
CDR-targeted approaches. For patients where the Cell Danger Response is a significant driver, interventions that support purinergic signaling normalization and allow cells to progress through the healing cycle are directly relevant to PEM. Reducing CDR activation reduces the hair-trigger sensitivity to exertion that characterizes severe PEM.
Careful sequencing. None of these interventions operates in isolation. PEM in Long COVID typically reflects multiple simultaneous mechanisms, and the clinical art is in identifying which mechanisms are dominant in a given patient and addressing them in the right sequence. A patient whose primary PEM driver is microclotting needs a different initial emphasis than a patient whose primary driver is MCAS-mediated immune activation after exercise.
What We Tell Our Patients
At Leading Edge Clinic, the practical guidance we give patients with significant PEM is this:
PEM is a real biological phenomenon with measurable cellular and vascular causes. It is not a symptom you can push through. Attempting to do so, without first addressing the underlying biology that is causing it, will not improve your condition… it will damage it.
However, there is good news. Your current energy envelope is not a permanent ceiling. It is a reflection of your current biological state. As we work on the underlying mechanisms (microclotting, immune dysregulation, CDR, mitochondrial function) your energy envelope will expand. We have seen it over and over. But that expansion has to come from biology improving, not from forcing activity in a system that isn’t ready for it.
This process takes time. It is non-linear. There will be weeks that feel like setbacks. Honest pacing and the discipline to stay within your current envelope even when you feel temporarily better is one of the most important things you can do to protect your recovery trajectory.
Recovery from PEM-dominated Long COVID is one of the slower trajectories we manage, and one of the most satisfying when it happens. Patients who have been bed-bound or housebound for years have regained meaningful function. But that recovery almost always required first stopping the cycle of crash and partial recovery that graded exercise therapy perpetuates, and replacing it with intelligent, mechanistically-informed clinical management.
If you’re interested in receiving care for your PEM, you can register here.
Leading Edge Clinic specializes in Long COVID, Post-Vaccine Syndrome, and complex post-infectious illness. Dr. Pierre Kory, Scott Marsland, FNP-C, and the rest of our clinical team have treated more than 3,500 patients, many who suffer with PEM. We see patients in all 50 states via telehealth.
This article is for educational purposes and does not constitute medical advice.
Key References
- Appelman B, Charlton BT, Goulding RP, et al. Muscle abnormalities worsen after post-exertional malaise in Long COVID. Nat Commun. 2024;15:17. https://doi.org/10.1038/s41467-023-44432-3
- Charlton BT, Goulding RP, Jaspers RT, et al. Skeletal muscle adaptations and post-exertional malaise in Long COVID. Trends Endocrinol Metab. 2025;36(7):614–622. https://doi.org/10.1016/j.tem.2024.11.008
- Aschman T, et al. Post-COVID exercise intolerance is associated with capillary alterations and immune dysregulations in skeletal muscles. Acta Neuropathol Commun. 2023;11:193. https://doi.org/10.1186/s40478-023-01662-2
- Towards an understanding of physical activity-induced post-exertional malaise: microvascular alterations and immunometabolic interactions in post-COVID and ME/CFS. PMC. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11825644/
- Letter to Nature: Graded exercise therapy should not be recommended for Long COVID patients with PEM. 2024. https://meassociation.org.uk/2024/01/nature-get-should-not-be-recommended-for-patients-with-pem/
- Vink M, Vink-Niese A. CBT and graded exercise therapy studies have proven that ME/CFS and Long COVID are physical diseases. Front Hum Neurosci. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11814198/