Long Covid vs Post-Vaccine Syndrome: What’s the Difference?
If you’re experiencing persistent fatigue, brain fog, heart palpitations, or exercise intolerance months after either COVID-19 infection or COVID-19 vaccination, you’re not alone — and you’re probably confused about what’s actually happening in your body.
At Leading Edge Clinic, we’ve treated over 3,500 patients with spike protein-related illness. The single most common question we hear is: “Is this Long Covid, or is this from the vaccine?”
The answer matters — not because the treatments are dramatically different (they’re not), but because understanding what’s driving your symptoms helps you find the right care and validates your experience when so many providers are dismissive.
Here’s what you need to know.
The Core Similarity: Both Are Spike Protein Illnesses
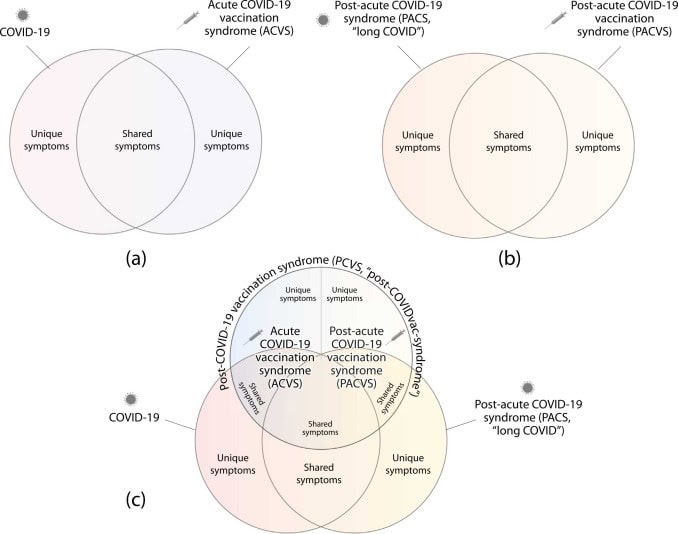
Before we talk about differences, let’s establish the most important thing: Long Covid and Post-Vaccine Syndrome share the same underlying pathology.
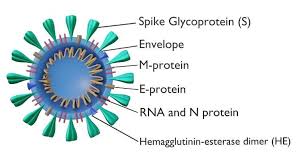
Both conditions are driven by the SARS-CoV-2 spike protein — the component of the virus responsible for binding to human cells and triggering immune response. In Long Covid, the spike protein comes from the virus itself. In Post-Vaccine Syndrome, it comes from the mRNA or adenovirus vaccines designed to teach your immune system to recognize that same spike protein.
The spike protein, regardless of its source, can cause:
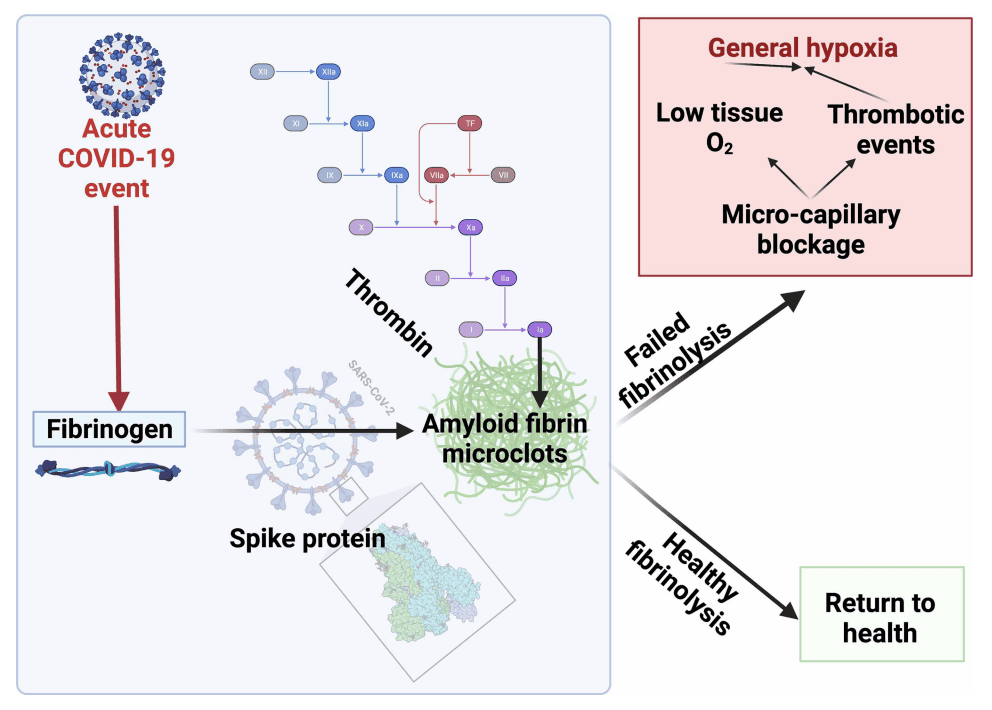
- Microclotting — tiny blood clots that reduce oxygen delivery to tissues and organs
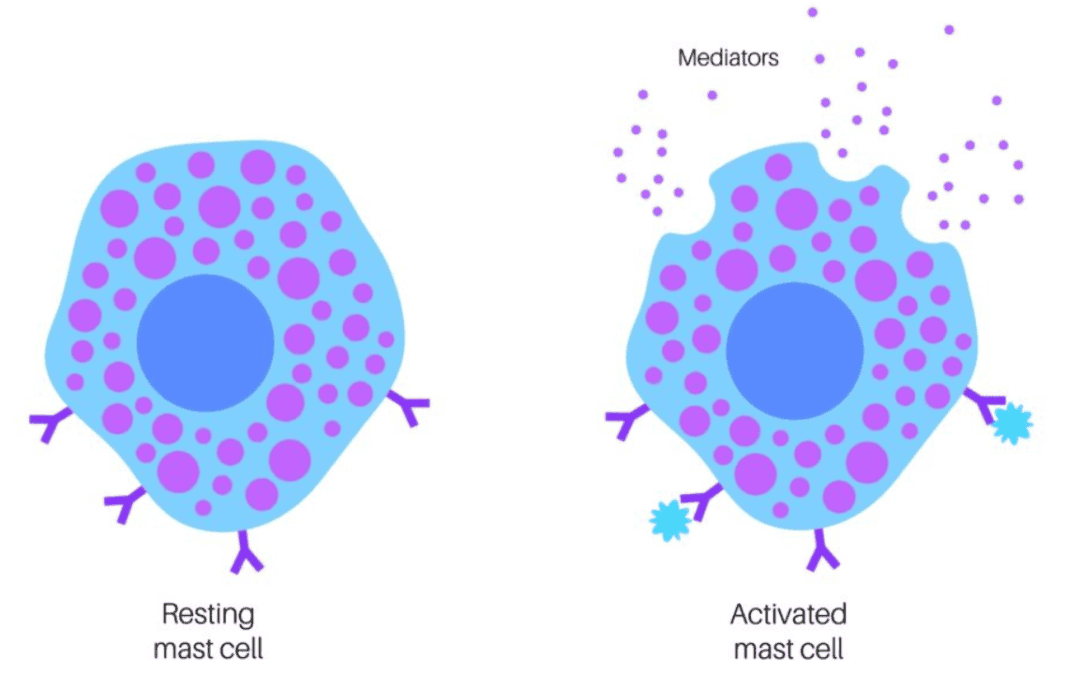
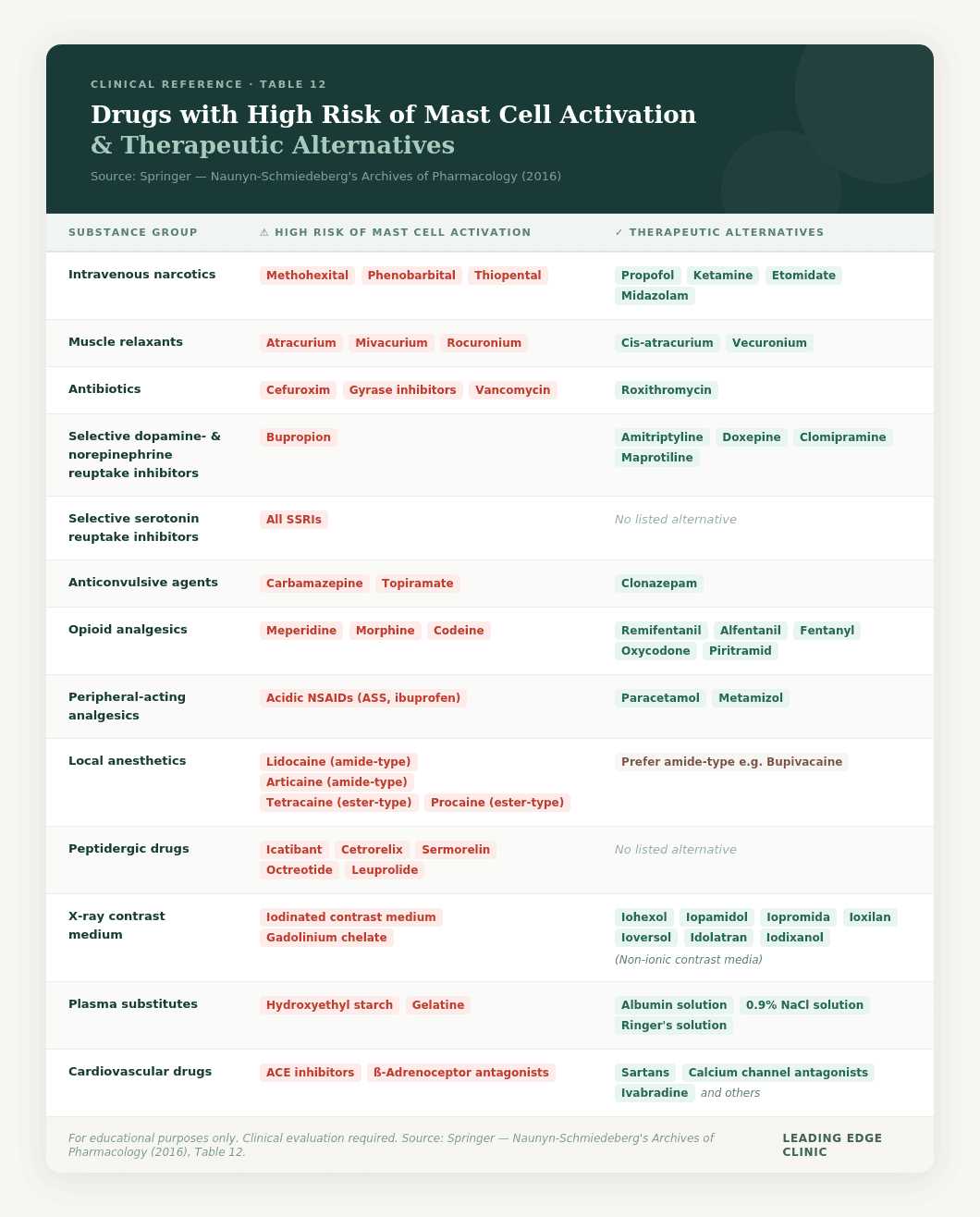
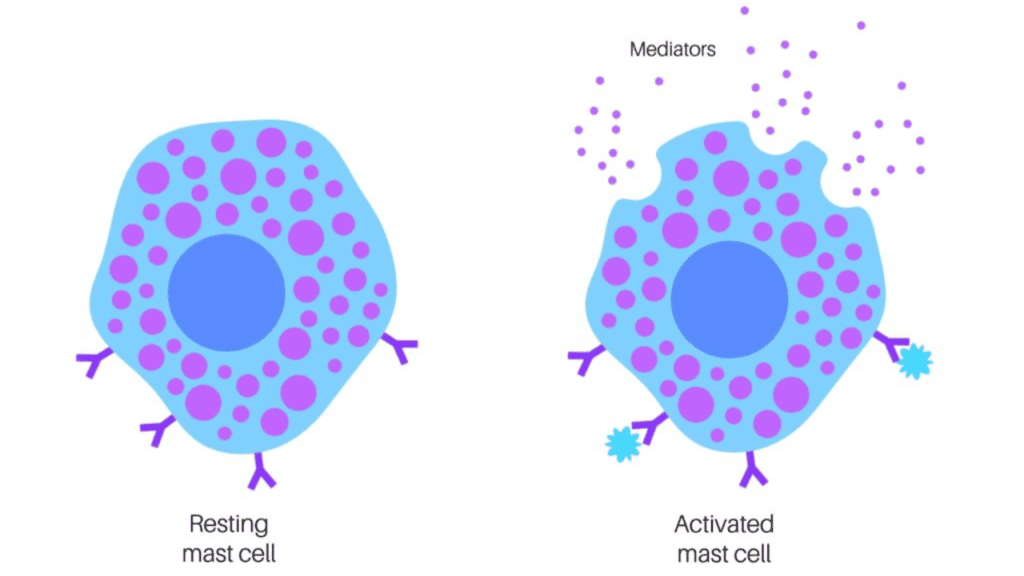
- Mast Cell Activation Syndrome (MCAS) — immune cells releasing histamine and inflammatory mediators inappropriately
- Immune dysregulation — autoimmune reactions, persistent inflammation, and impaired pathogen clearance
- Mitochondrial dysfunction — reduced cellular energy production, leading to profound fatigue and post-exertional malaise (PEM)
- Autonomic nervous system dysfunction — POTS (Postural Orthostatic Tachycardia Syndrome), blood pressure instability, and temperature dysregulation
This is why the symptom overlap between Long Covid and Post-Vaccine Syndrome is so extensive. You’re dealing with the same underlying mechanisms.
Key Differences Between Long Covid and Post-Vaccine Syndrome
While the pathophysiology overlaps, there are meaningful differences in how these conditions develop, how they’re perceived by the medical community, and what patients typically experience.
1. Trigger Event
Long Covid:
Symptoms persist for 3+ months following acute SARS-CoV-2 infection. Most Long Covid patients can point to a specific COVID-19 illness — sometimes mild, sometimes severe — that preceded their chronic symptoms.
Post-Vaccine Syndrome (PACVS):
Symptoms develop days, weeks, or even months after receiving an mRNA (Pfizer, Moderna) or adenovirus (J&J, AstraZeneca) COVID-19 vaccine. Some patients experience immediate reactions (within hours to days), while others notice a gradual onset of symptoms over weeks.
2. Onset Timing
Long Covid:
By definition, Long Covid symptoms last at least 3 months post-infection. Many patients experience a biphasic pattern — they recover from the acute infection, feel better for a period, then crash weeks later with persistent symptoms.
Post-Vaccine Syndrome:
Onset can be more variable. Some patients develop symptoms immediately after vaccination (within 24-72 hours). Others experience a delayed onset, with symptoms appearing 2-4 weeks post-vaccination, or even after the second or third dose rather than the first.
3. Prevalence
Long Covid:
Estimates vary widely, but research suggests 10-30% of people infected with SARS-CoV-2 develop some form of Long Covid. The condition is now widely recognized (though still poorly understood) by mainstream medicine.
Post-Vaccine Syndrome:
Exact prevalence is unknown, many news outlets report Post-Vaccine Syndrome appears to be less common than Long Covid. However, underreporting is a significant issue — many patients who develop symptoms post-vaccination are told their symptoms are unrelated, or due to Covid Infection, which discourages official reporting and makes true prevalence difficult to estimate.
4. Medical Recognition and Acceptance
Long Covid:
Mainstream medicine now acknowledges Long Covid as a real condition. The NIH has funded Long Covid research, the CDC tracks it, and most physicians — even if they don’t know how to treat it — at least believe it exists.
Post-Vaccine Syndrome:
This is where the experiences of Long Covid and Post-Vaccine Syndrome patients diverge most sharply. Post-Vaccine Syndrome is frequently dismissed by conventional medicine. Patients are often told:
- “The vaccine is safe and effective — your symptoms can’t be related.”
- “It’s anxiety.”
- “It’s a coincidence.”
- “Your labs are normal, so nothing is wrong.”
For the first time, mainstream medicine has begun to acknowledge Post-Vaccine Syndrome. A 2024 Yale study formally recognized what our patients have known for years: vaccine-associated Long Covid-like illness is real, measurable, and distinct from Long Covid caused by infection.
But clinical recognition still lags far behind the research. Most Post-Vaccine Syndrome patients spend months or years seeking validation before finding a provider who takes them seriously.
5. Symptom Presentation
The symptoms themselves are remarkably similar, but there are some patterns we’ve observed across thousands of patients:
Long Covid patients more commonly report:
- Loss of taste or smell (especially early in the pandemic)
- Respiratory symptoms (shortness of breath, chronic cough)
- Gradual, progressive worsening over months
Post-Vaccine Syndrome patients more commonly report:
- Sudden, acute onset of symptoms (within days of vaccination)
- Severe neurological symptoms (neuropathy, tremors, cognitive impairment)
- Cardiovascular symptoms (chest pain, pericarditis, myocarditis-like symptoms)
- Menstrual irregularities (particularly after mRNA vaccines)
These are tendencies, not rules. We’ve seen every presentation in both patient populations. The symptom overlap is far more significant than the differences.
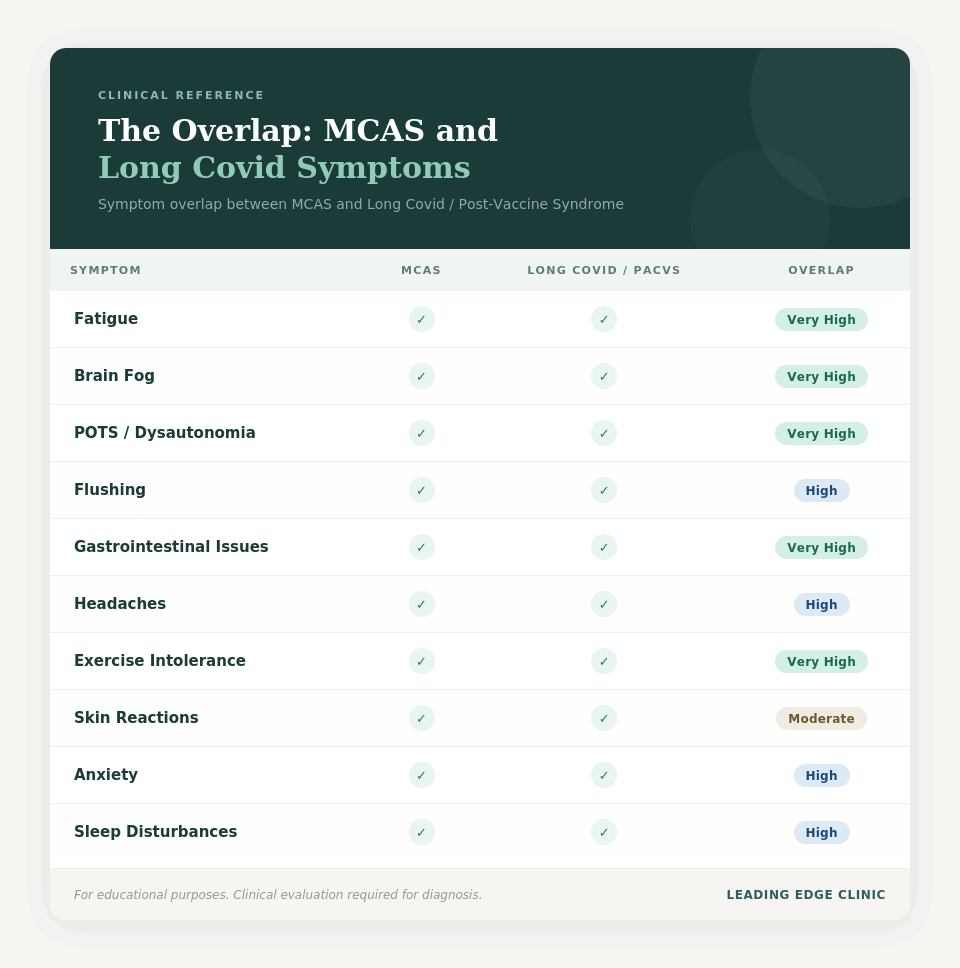
Symptom Comparison: Long Covid vs Post-Vaccine Syndrome
The table below shows which symptoms are common to both conditions, and which tend to be more prominent in one versus the other. Remember: these are patterns we’ve observed across thousands of patients, not absolute rules. Every patient is unique.
| Symptom | Long Covid | Post-Vaccine Syndrome | Overlap | Notes |
|---|---|---|---|---|
| Severe Fatigue | ✓ | ✓ | Very High | Present in >90% of both populations |
| Brain Fog | ✓ | ✓ | Very High | Cognitive impairment, memory issues, difficulty concentrating |
| Post-Exertional Malaise (PEM) | ✓ | ✓ | Very High | Symptom worsening after physical or mental exertion |
| POTS / Dysautonomia | ✓ | ✓ | Very High | Heart rate increases, dizziness upon standing |
| Heart Palpitations | ✓ | ✓ | Very High | Often worse at night or with positional changes |
| Shortness of Breath | ✓✓ | ✓ | High | Slightly more common in Long Covid |
| Exercise Intolerance | ✓ | ✓ | Very High | Inability to return to pre-illness activity levels |
| Sleep Disturbances | ✓ | ✓ | High | Insomnia, unrefreshing sleep, sleep maintenance issues |
| Anxiety / Depression | ✓ | ✓ | High | Can be physiological (histamine, inflammation) not just psychological |
| Headaches / Migraines | ✓ | ✓ | High | Often treatment-resistant |
| Neuropathy / Nerve Pain | ✓ | ✓✓ | High | Tingling, burning, numbness; more acute in PACVS |
| Tremors | ✓ | ✓✓ | Moderate | More commonly reported in PACVS patients |
| Chest Pain | ✓ | ✓✓ | High | May indicate pericarditis or myocarditis (more common post-vaccine) |
| GI Issues | ✓ | ✓ | High | Nausea, diarrhea, constipation, GERD |
| Tinnitus (Ringing in Ears) | ✓ | ✓ | Moderate | Persistent ringing or buzzing |
| Loss of Taste/Smell | ✓✓ | ✓ | Moderate | Much more common in Long Covid, especially early pandemic |
| Skin Rashes / Hives | ✓ | ✓ | Moderate | Often MCAS-related |
| Temperature Dysregulation | ✓ | ✓ | High | Inability to regulate body temperature, chills, sweats |
| Menstrual Irregularities | ✓ | ✓✓ | High | Heavy periods, irregular cycles; more pronounced post-mRNA vaccines |
| Hair Loss | ✓ | ✓ | Moderate | Telogen effluvium pattern |
| Joint Pain | ✓ | ✓ | High | Migratory or persistent arthralgia |
| Muscle Pain | ✓ | ✓ | High | Myalgia, often widespread |
| Vision Changes | ✓ | ✓ | Moderate | Blurred vision, light sensitivity, floaters |
Key:
✓ = Symptom present
✓✓ = Symptom more prominent in this condition
Overlap: Very High (>80% of both populations), High (60-80%), Moderate (40-60%)
What This Table Shows
The overwhelming similarity in symptom presentation is what makes distinguishing Long Covid from Post-Vaccine Syndrome so difficult — and why your timeline and trigger event (infection vs. vaccination) are often the only reliable differentiators.
If you’re experiencing multiple symptoms from this table and conventional medicine has told you “nothing is wrong” because your labs are normal, you’re not imagining it. These are real, measurable manifestations of spike protein pathology — and they require specialized treatment.
Why the Overlap Exists: Spike Protein Pathology
Whether spike protein enters your body via infection or vaccination, it triggers similar downstream effects:
Microclotting
The spike protein binds to ACE2 receptors on the endothelium (blood vessel lining), causing inflammation and microclot formation. These tiny clots reduce blood flow to tissues, leading to:
- Brain fog (reduced oxygen to brain)
- Exercise intolerance (reduced oxygen to muscles)
- Shortness of breath (impaired gas exchange in lungs)
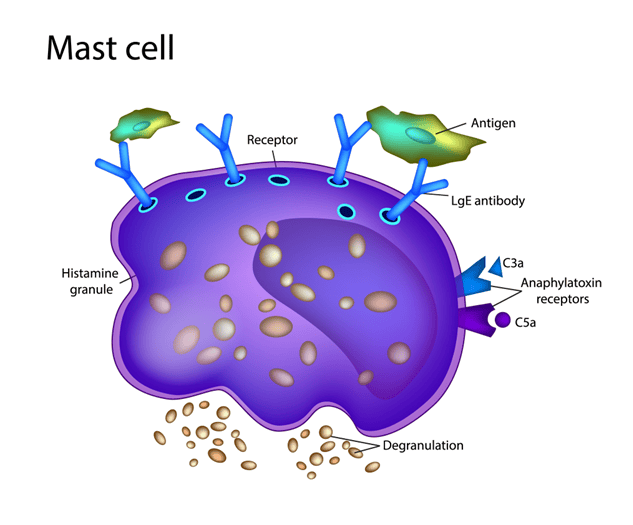
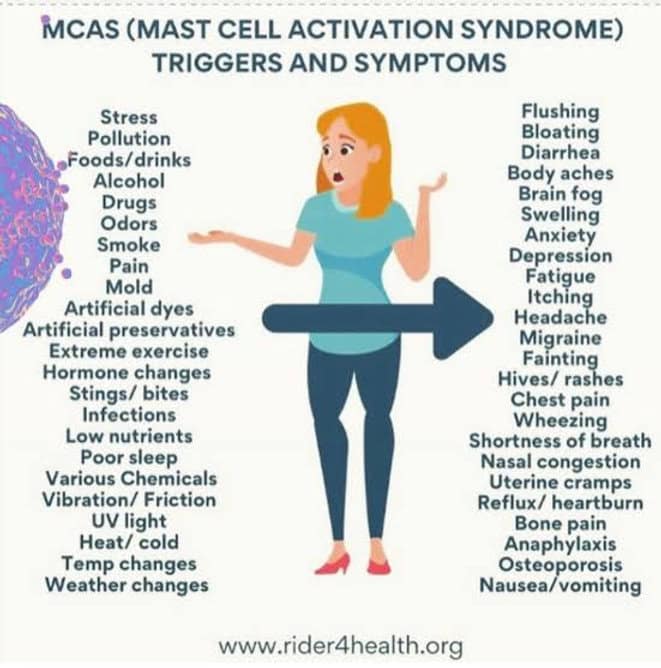
Mast Cell Activation
Spike protein triggers mast cells to degranulate, releasing histamine and other inflammatory mediators. This causes:
- Flushing
- Heart palpitations
- Digestive issues
- Skin reactions
- Anxiety and hypervigilance (histamine affects the brain)
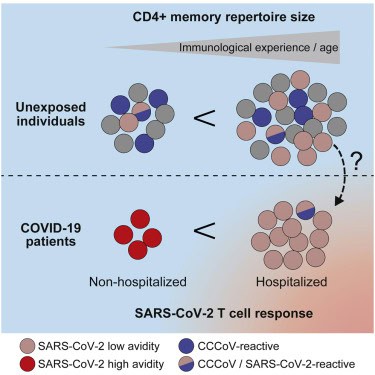
Immune Dysregulation
The immune system becomes overactive in some areas (autoimmunity, persistent inflammation) and underactive in others (viral reactivation of Epstein-Barr, HHV-6, etc.). The lack of balance in the immune system can be referred to as “dysregulation”, rather than only referring to it as oceractivation or underactivation. The end result is typically immune exhaustion, and can manifest as lower CD4 T-Cell counts).
Mitochondrial Dysfunction
Spike protein damages mitochondria — the energy-producing organelles in your cells — leading to:
- Severe fatigue
- Post-exertional malaise (PEM)
- Exercise intolerance
- Cognitive dysfunction
This shared pathology is why treatment approaches for Long Covid and Post-Vaccine Syndrome are fundamentally the same.
Treatment Implications: Why the Distinction Matters (and Doesn’t)
Why It Doesn’t Matter Much for Treatment
The good news: if you have spike protein illness, the treatment approach is similar regardless of the source.
Both conditions respond to protocols that address:
- Spike protein clearance
- Microclotting reduction
- MCAS stabilization
- Inflammatory response reduction
- Clearance of senescent cells
- Cell Danger Response modulation
- Immune modulation
- Mitochondrial support
- Viral reactivation management
- Foundational health approaches
At Leading Edge Clinic, we use the same foundational approaches for both Long Covid and Post-Vaccine Syndrome patients. The personalization comes from your specific symptom presentation, not from which spike protein source triggered your illness.
Why It Does Matter
Even though treatment is similar, the distinction matters for three reasons:
1. Finding a Provider Who Believes You
Long Covid patients can usually find a provider willing to acknowledge their condition. Post-Vaccine Syndrome patients face significantly more dismissal. Knowing what you’re dealing with helps you seek care from providers (like us) who specialize in both.
2. Understanding Your Timeline
Post-Vaccine Syndrome patients often experience more acute, sudden onset — which can be frightening. Knowing this is a recognized pattern helps contextualize your experience.
3. Preventing Re-Exposure
Both Long Covid and Post-Vaccine Syndrome patients need to be cautious about reinfection (which can worsen symptoms). We know that continuous spike protein exposure will further trigger related symtpoms, and increase the number of senescent cells. Understanding your trigger helps you make informed decisions about future exposures.
How Leading Edge Clinic Treats Both Conditions
We’ve treated over 3,500 patients with spike protein illness — both Long Covid and Post-Vaccine Syndrome. Here’s how we approach care:
Comprehensive Initial Evaluation
We don’t care whether your spike protein came from infection or vaccination. We care about:
- Which body systems are affected (cardiovascular, neurological, immune, etc.)
- The severity of your symptoms
- Your specific symptom triggers
- Any viral reactivations or co-infections
- Your prior treatment history and what’s worked (or hasn’t)
Personalized Treatment Plans
Our protocols address:
- Spike protein burden reduction
- Microclotting and vascular inflammation
- Mast cell stabilization (if MCAS is present)
- Immune system rebalancing
- Mitochondrial function restoration
- System inflammation reduction
- Cell Danger Response modulation
- Clearing senescent cells
- Dealing with prion-like domains
- Symptom management (POTS, brain fog, fatigue, etc.)
Proactive RN Follow-Up
You’re not left on your own between appointments. Our Registered Nurses check in every other week to monitor your response, adjust protocols, and escalate concerns to providers immediately if something isn’t working.
Telehealth in All 50 States
We see patients nationwide via secure telehealth. You don’t need to live near us to receive specialized care.
Learn more about our approach:
The Bottom Line
Long Covid and Post-Vaccine Syndrome are not identical conditions, but they share the same underlying pathology: spike protein-driven illness.
The key differences are:
- Trigger: Infection vs. vaccination
- Onset timing: Gradual vs. often more acute
- Medical recognition: Acknowledged vs. frequently dismissed
But the similarities far outweigh the differences:
- Both involve spike protein pathology
- Both cause microclotting, MCAS, immune dysregulation, chronic Cell Danger Response, senescent cell cycle, mitochondrial dysfunction
- Both respond to similar treatment protocols
- Both require specialized care from providers who understand spike protein illness
If you’re struggling with persistent symptoms after COVID-19 infection or vaccination, you’re not imagining it. You’re not alone. And there are providers who can help.
Suspect you have Long Covid or Post-Vaccine Syndrome?
Register to become a patient or learn more about our approach.
Frequently Asked Questions
Can you have both Long Covid and Post-Vaccine Syndrome?
Yes. Some patients develop Long Covid from an initial infection, then experience worsening symptoms after vaccination. Others develop Post-Vaccine Syndrome first, then experience symptom escalation after a subsequent COVID-19 infection. The spike protein exposures are cumulative, as is the build up of senescent cells
How do I know which one I have?
The timeline is your best clue. If your symptoms started within days to weeks to months of vaccination (and you hadn’t recently had COVID), it’s likely Post-Vaccine Syndrome. If symptoms followed a documented COVID infection and persisted for months, it’s likely Long Covid. If you’ve had multiple exposures (infection + vaccines), you may have elements of both.
Will my doctor test me to determine which one it is?
There’s no single test that definitively distinguishes Long Covid from Post-Vaccine Syndrome. Diagnosis is clinical — based on your history, timeline, and symptom pattern. Some providers order microclot testing, inflammatory markers, or immune panels, but these show similar abnormalities in both conditions.
Does it matter for insurance coverage?
In the U.S., both conditions are generally treated the same by insurance (though coverage for integrative treatments is often limited regardless). The diagnosis code used may vary, but treatment coverage depends more on the specific interventions prescribed than on whether the spike protein came from infection or vaccination.
Are the outcomes different for Long Covid vs. Post-Vaccine Syndrome?
We don’t have enough long-term data to say definitively. Anecdotally, we have seen Post-Vaccine Syndrome patients typically have more severe presentations, with a longer road to recovery. However, this isn’t always the case. The biggest predictor of outcome isn’t the spike protein source — it’s how quickly patients receive appropriate treatment and how severe their initial presentation was.
About the Author:
This article was written by the clinical team at Leading Edge Clinic, which has treated over 3,500 patients with Long Covid, Post-Vaccine Syndrome, and related spike protein illnesses. Our providers include Dr. Pierre Kory (MD, MPA), Scott Marsland (FNP-C), India Scott (FNP-C), and other specialists in complex chronic illness.
Medical Disclaimer:
This article is for educational purposes only and is not a substitute for personalized medical advice. If you’re experiencing persistent symptoms after COVID-19 infection or vaccination, please consult with a healthcare provider experienced in treating spike protein-related illness.