How to Know If You Have Post-Vaccine Syndrome: 7 Key Warning Signs
If you’re experiencing persistent, unexplained symptoms that started shortly after your COVID-19 vaccination, you’re not alone, and you’re not imagining it. Post-Vaccine Syndrome (PVS), also called Post-Acute COVID-19 Vaccination Syndrome (PACVS), is an increasingly recognized condition affecting a small percentage of vaccine recipients.
The challenge? Many doctors aren’t familiar with PVS, dismissing symptoms as anxiety or “normal” post-vaccination effects. This leaves patients confused, undiagnosed, and without the specialized care they need.
This guide will help you recognize the warning signs of Post-Vaccine Syndrome, understand how it differs from acute vaccine side effects, and know when to seek specialized medical care.
What Is Post-Vaccine Syndrome?
Post-Vaccine Syndrome is a chronic condition characterized by persistent, multi-system symptoms that develop shortly after COVID-19 vaccination and last for weeks, months, or even years.
According to research from Yale University’s LISTEN Study, PVS patients experience debilitating symptoms that begin within hours to days of vaccination, with a median onset of just three days, and continue long after normal vaccine side effects should have resolved. In our own experience, these symptoms can even develop months after mRNA vaccination, as the condition may also appear through accumulation of spike protein.
The Numbers You Should Know
- Symptom onset: Yale study shows typically 1-8 days after vaccination (median: 3 days); but our observations also indicate weeks, to months
- Duration: Symptoms lasting 4 weeks or longer (many patients: months to years)
- Prevalence: Again, based on Yale data, estimated 0.02-2% of vaccinated individuals; however, we believe this number to be higher based on our patient demographics (70% Post-Vaccine Syndrome versus 30% Long Haul Covid)
- Demographics: 80% female, median age 46 years (though it can affect anyone)
- Severity: 71-80% of patients report significant impact on daily functioning
Important: PVS is real, recognized by researchers at institutions like Yale, NIH, and leading medical centers. Most importantly, it’s treatable with specialized care.
Understanding the Timeline: When Do PVS Symptoms Start?
One of the most important diagnostic clues for Post-Vaccine Syndrome is when your symptoms began.
Acute Vaccine Side Effects:
- Onset: Within 24-48 hours
- Duration: 2-3 days maximum
- Severity: Mild to severe
- Examples: Anaphylactic episodes, bloot clots, heart attack/stroke, etc…
Post-Vaccine Syndrome:
- Onset: Hours to days to months after vaccination
- Duration: 4+ weeks minimum (often months or years)
- Severity: Moderate to severe, often debilitating
- Example: A constellation of multi-system symptoms, as opposed to an acute injury
According to the Yale LISTEN Study of 241 PVS patients:
- Median symptom onset: 3 days after vaccination
- Range: 1-8 days (though some patients report onset within hours)
- Duration at time of study: Median 595 days (nearly 20 months)
Why timing matters: A temporal relationship between vaccination and symptom onset, especially when symptoms start within days, is a key diagnostic indicator that helps distinguish PVS from other conditions. While the Yale study looked at patients who experienced PVS symptoms within days, we also know the temporal association can be drawn out months.
The 7 Core Warning Signs of Post-Vaccine Syndrome
If you’re experiencing several of these symptoms that started shortly after vaccination and have lasted more than 4 weeks, you may have Post-Vaccine Syndrome.
Warning Sign #1: Exercise Intolerance (Affects 71% of Patients)
What it looks like:
- Unable to perform physical activities you could do easily before vaccination
- Severe exhaustion after minimal exertion (walking up stairs, grocery shopping, light housework)
- Recovery takes days or weeks, not hours
- “Crashes” after activity that leave you bedbound
How it differs from normal fatigue:
- Normal post-vaccine fatigue: Tired but can still function; improves with rest and time
- PVS exercise intolerance: Disproportionate exhaustion; worsens with activity; doesn’t improve with rest and is ongoing
Real patient example: “I used to go to the gym five days a week. Now I can’t walk to my mailbox without needing to lie down for hours afterward. It’s been 8 months since my booster.”
This is called Post-Exertional Malaise (PEM) and is one of the hallmark features of PVS. If you notice that physical or mental exertion triggers severe exhaustion that lasts for days, this is a significant warning sign.
Warning Sign #2: Excessive, Persistent Fatigue (Affects 69% of Patients)
What it looks like:
- Overwhelming exhaustion that doesn’t improve with sleep or rest
- Feeling exhausted upon waking, even after a full night’s sleep
- Fatigue that interferes with work, social life, and basic daily activities
- Described as “bone-deep” or “crushing” fatigue
How it differs from normal tiredness:
- Normal tiredness: Improves with rest; comes and goes; doesn’t prevent basic functioning
- PVS fatigue: Constant; severe; doesn’t respond to rest; prevents normal activities
Duration matters: Acute post-vaccine fatigue resolves within days. If your fatigue has lasted 4+ weeks and shows no signs of improving, this could indicate PVS.
Associated symptoms:
- Unrefreshing sleep
- Need to rest frequently during the day
- Can’t maintain previous work schedule
- Simple tasks (showering, cooking) become exhausting
Warning Sign #3: Neurological Symptoms (Affects 63% of Patients Each)
PVS frequently causes neurological symptoms across three categories:
A. Brain Fog and Cognitive Issues (63%)
- Difficulty concentrating or focusing
- Memory problems (forgetting words, appointments, recent conversations)
- Feeling “mentally slow” or confused
- Trouble processing information or making decisions
- Feeling “disconnected” or in a mental haze
B. Numbness and Tingling (63%)
- Pins-and-needles sensations in hands, feet, or other body parts
- Numbness that comes and goes or persists
- Areas of reduced sensation
- Feeling of “electric shocks”
C. Neuropathy (63%)
- Burning sensations
- Shooting pains
- Sensitivity to touch
- Pain in extremities
- Small fiber neuropathy symptoms
Other neurological symptoms reported:
- Visual disturbances (floaters, light sensitivity, scintillating scotoma)
- Headaches or migraines (often severe and persistent)
- Dizziness or vertigo
- Ringing in ears (tinnitus)
Why this matters: When neurological symptoms appear shortly after vaccination and persist for weeks or months, especially when combined with other PVS symptoms, this strongly suggests Post-Vaccine Syndrome rather than coincidental neurological issues.
Warning Sign #4: Dysautonomia and Cardiovascular Symptoms
What is dysautonomia? Dysfunction of the autonomic nervous system, which controls involuntary bodily functions like heart rate, blood pressure, and digestion.
Common cardiovascular symptoms in PVS:
- Heart palpitations: Feeling your heart racing, pounding, or skipping beats
- Tachycardia: Elevated heart rate, especially when standing or with minimal activity
- Orthostatic intolerance: Dizziness, lightheadedness, or near-fainting when standing up
- POTS-like symptoms: Postural Orthostatic Tachycardia Syndrome symptoms (heart rate increases 30+ bpm upon standing)
- Blood pressure irregularities: Sudden drops or spikes
- Chest discomfort: Not typical angina, but feeling of pressure or discomfort
How common is this? Research shows that dysautonomia symptoms—particularly orthostatic intolerance and tachycardia—are frequently reported by PVS patients and often overlap with POTS (Postural Orthostatic Tachycardia Syndrome).
Red flags requiring immediate medical attention:
- Severe chest pain
- Shortness of breath at rest
- Heart rate over 120 bpm at rest
- Fainting or loss of consciousness
If you experience these emergency symptoms, seek immediate medical care or call 911.
Warning Sign #5: Sleep Disturbances
What it looks like:
- Insomnia despite being exhausted
- Waking frequently during the night
- Unrefreshing sleep (waking up as tired as when you went to bed)
- Disrupted sleep patterns or circadian rhythm issues
- Difficulty falling asleep or staying asleep
Why sleep problems matter in PVS: Sleep disturbances in Post-Vaccine Syndrome aren’t just “can’t sleep because I’m stressed.” They’re often part of the autonomic nervous system dysfunction that characterizes the condition.
Many PVS patients report that they’re utterly exhausted but cannot sleep well, creating a vicious cycle of fatigue and poor rest.
Warning Sign #6: Multi-System Symptoms
Post-Vaccine Syndrome often affects multiple body systems simultaneously. Here are commonly reported symptoms:
Gastrointestinal Issues:
- Nausea
- Significant weight loss or gain (without dietary changes)
- Loss of appetite or changes in appetite
- Digestive problems
- Abdominal discomfort
Musculoskeletal Symptoms:
- Muscle pain (myalgia) or weakness
- Joint pain or stiffness
- Muscle twitching or fibrillations
- Temperature-sensitive muscle pain (worsens with cold or heat)
Temperature Regulation Problems:
- Inability to regulate body temperature
- Feeling excessively hot or cold
- Low-grade fevers that come and go
- Chills or sweating unrelated to activity
Immune System Issues:
- Frequent infections or illness
- Slow healing
- Reactivation of viruses (e.g., Epstein-Barr Virus – found in many PVS patients)
The multi-system nature is a key diagnostic feature. If you’re experiencing symptoms across several different body systems that all started around the time of vaccination, this pattern strongly suggests PVS.
Warning Sign #7: Psychological and Emotional Impact
Important distinction: The psychological symptoms in PVS are a result of the physical illness, not psychosomatic or “all in your head.”
According to the Yale LISTEN Study, in the week before completing their survey, PVS patients reported:
- Anxiety: 76% of patients
- Depression: 76%
- Feelings of helplessness: 80%
- Feelings of hopelessness: 72%
- Overwhelming worry: 81%
- Feeling fearful: 82%
Why these feelings occur:
- Actual physiological changes to the body (ie: brain inflammation)
- Chronic illness is emotionally devastating
- Many doctors dismiss or don’t recognize PVS
- Patients often feel gaslit or not believed
- Loss of previous quality of life
- Uncertainty about recovery
- Inability to work or maintain normal activities
This is NOT psychosomatic illness. The psychological symptoms are the natural emotional response to living with a debilitating, poorly recognized chronic condition. Multiple studies have identified biological markers (elevated interleukins, receptor antibody changes, persistent spike protein) that confirm PVS is a somatic (physical) condition.
How Post-Vaccine Syndrome Differs from Acute Vaccine Side Effects
It’s crucial to distinguish between acute vaccine reactions and Post-Vaccine Syndrome.
Acute Vaccine Side Effects
| Characteristic | Acute Side Effects |
|---|---|
| Onset | Within 24-48 hours |
| Duration | 2-3 days maximum |
| Symptoms | Fever, chills, fatigue, headache, sore arm, anaphylaxis, blood clots, stroke, etc… |
| Severity | Mild to severe |
| Impact | Can function with some discomfort, or can be deadly |
| Resolution | Complete recovery within days, or long-lasting effects from a severe acute episode |
Post-Vaccine Syndrome
| Characteristic | Post-Vaccine Syndrome |
|---|---|
| Onset | Hours to weeks to months |
| Duration | 4+ weeks minimum (often months/years) |
| Symptoms | Multi-system: neurological, cardiovascular, fatigue, pain, cognitive issues |
| Severity | Moderate to severe, often debilitating |
| Impact | Significant impairment of daily functioning; many unable to work |
| Resolution | Does not resolve on its own; requires specialized treatment |
The key difference: Post-Vaccine Syndrome symptoms don’t improve over time without treatment. Some acute vaccine side effects resolve completely within days.
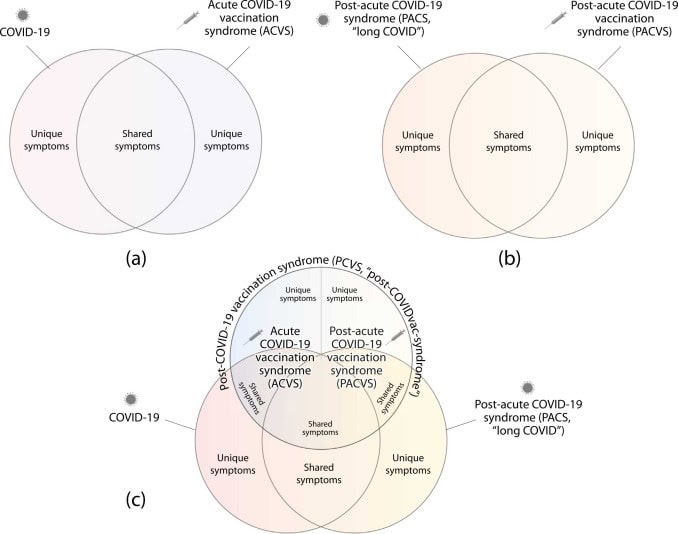
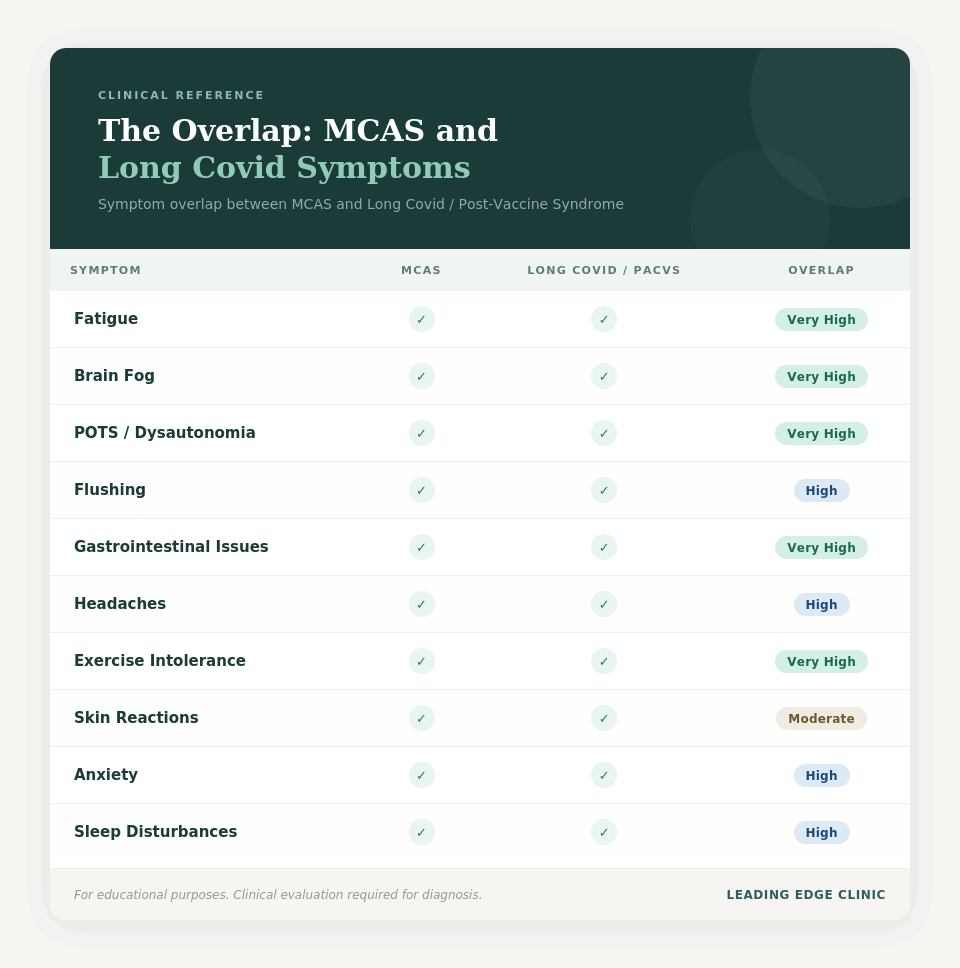
How Post-Vaccine Syndrome Differs from Long COVID
Many people—including doctors—confuse Post-Vaccine Syndrome with Long COVID because the symptoms are remarkably similar. We also believe this is why study after study says Post-Vaccine Syndrome is “rare”. However, there are key differences.
Key Differences:
Trigger:
- Long COVID: Follows COVID-19 infection
- PVS: Follows COVID-19 vaccination (without prior infection)
COVID Testing:
- Long COVID: History of positive COVID test or confirmed infection
- PVS: Negative COVID tests; no evidence of prior infection
Timing:
- Long COVID: Symptoms begin during or after COVID infection
- PVS: Symptoms begin vaccination
Spike Protein Source:
- Long COVID: Spike protein from actual SARS-CoV-2 virus
- PVS: Spike protein from vaccine (mRNA-induced production)
Important Overlap:
Both conditions involve:
- Persistent spike protein in the body
- Multi-system symptoms
- Exercise intolerance and post-exertional malaise
- Dysautonomia
- Cognitive issues
- Similar treatment approaches
What if I had COVID AND got vaccinated?
Some patients have overlapping exposures, which can complicate diagnosis, but not treatment. In these cases, a detailed timeline looks at:
- When did COVID infection occur?
- When did vaccination occur?
- When did symptoms start or significantly worsen?
Many patients report being relatively recovered from COVID but developing severe symptoms after vaccination, suggesting the vaccine triggered or exacerbated the condition.
For a detailed comparison of Long COVID and Post-Vaccine Syndrome, including symptom overlaps and how treatment differs, read our comprehensive guide: https://drpierrekory.com/blog/long-covid-vs-post-vaccine-syndrome-whats-the-difference/
The Diagnostic Challenge: Why PVS Is Often Missed
Post-Vaccine Syndrome is difficult to diagnose for several reasons:
1. No Single Definitive Test
Currently, there’s no single blood test or scan that definitively confirms PVS. Diagnosis is based on:
- Clinical presentation (symptoms)
- Temporal relationship to vaccination
- Ruling out other conditions
- Emerging biomarkers (when available)
2. Many Doctors Aren’t Familiar with PVS
Despite growing research from institutions like Yale, NIH, and leading medical centers, many physicians:
- Haven’t heard of Post-Vaccine Syndrome
- Don’t recognize the symptom pattern
- Dismiss symptoms as anxiety or stress
- Aren’t comfortable discussing vaccine-related adverse events
3. Symptoms Overlap with Other Conditions
PVS symptoms can mimic:
- ME/CFS (Myalgic Encephalomyelitis/Chronic Fatigue Syndrome)
- POTS (Postural Orthostatic Tachycardia Syndrome)
- Fibromyalgia
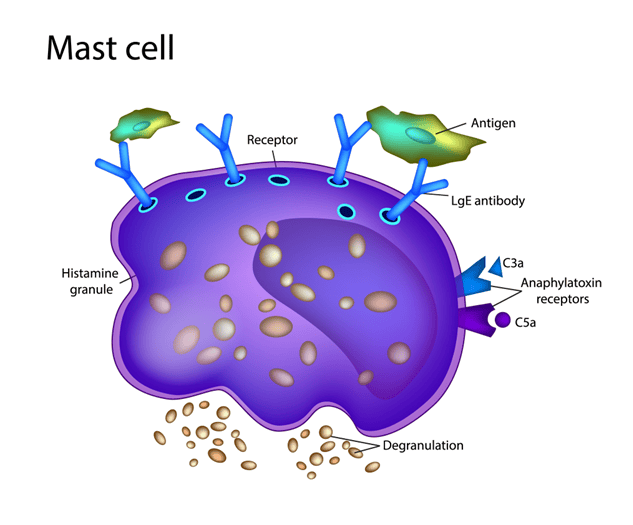
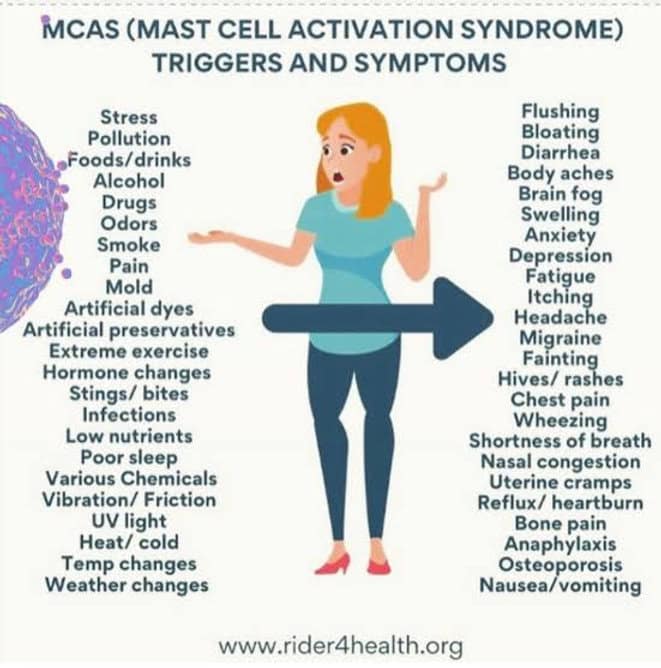
- MCAS (Mast Cell Activation Syndrome)
- Small fiber neuropathy
In fact, research shows that many PVS patients meet diagnostic criteria for one or more of these conditions.
4. Normal Test Results
Many PVS patients have normal or near-normal results on standard tests:
- Normal bloodwork
- Normal imaging (MRI, CT scans)
- Normal cardiac workup
- Normal neurological exams
This leads doctors to conclude “nothing is wrong” when, in reality, the standard tests aren’t measuring the right markers.
Emerging Diagnostic Markers for Post-Vaccine Syndrome
While there’s no single definitive test yet, research has identified several biological markers associated with PVS:
1. Persistent Spike Protein
Yale researchers found that some PVS patients have detectable spike protein in their blood more than 700 days (nearly 2 years) after vaccination.
Normal: Spike protein typically clears within days to weeks after vaccination.
PVS: Persistent spike protein suggests the body is unable to clear it normally, potentially triggering ongoing inflammation and symptoms.
What this study misses, and what our colleagues (such as Vedicinals) are researching, is spike protein persistence intraceullarly or in-tissue (Yale only looked at circulating). We believe strongly that uncovering spike protein prevalence in tissue will create a much stronger signal for both potential PVS and Long Covid
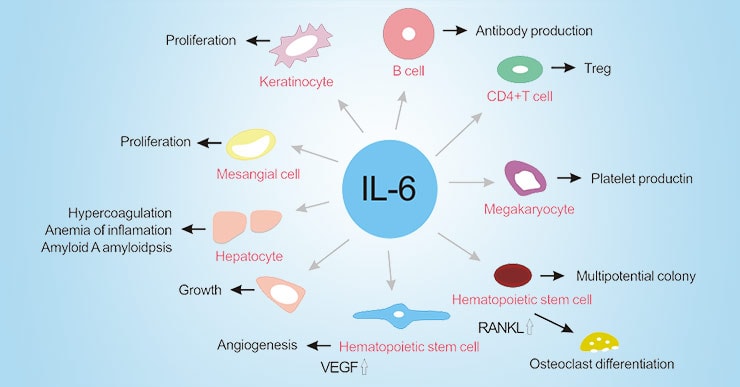
2. Elevated Inflammatory Markers
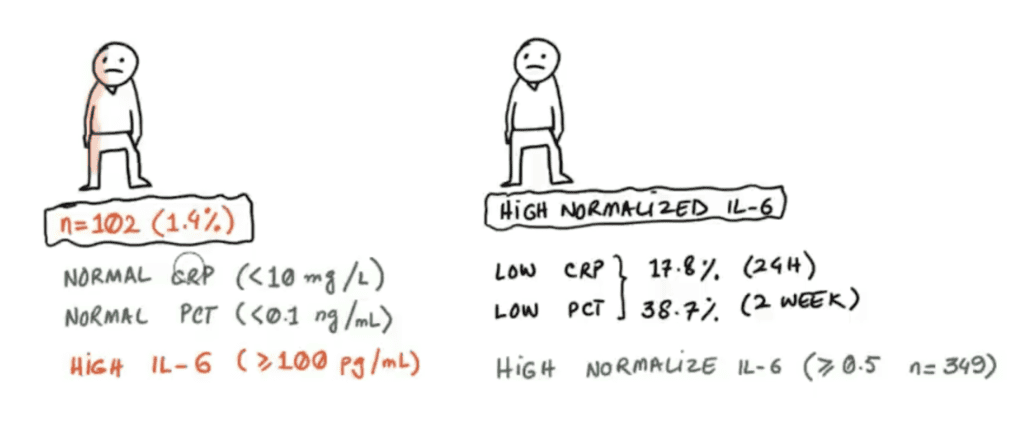
Studies have found that PVS patients often have:
- Elevated Interleukin-6 (IL-6): Found in over 80% of PVS patients
- Elevated Interleukin-8 (IL-8): Also found in over 80% of patients
- These cytokines indicate ongoing inflammation
3. Altered Receptor Antibodies
Research from Germany identified significant changes in specific receptor antibodies in PVS patients:
- Angiotensin II Type 1 Receptor (AT1R) antibodies: Increased in PVS
- Alpha-2B Adrenergic Receptor antibodies: Decreased in PVS
- Combined with IL-6, these markers can distinguish PVS from normal post-vaccination response with up to 90% accuracy
4. Epstein-Barr Virus (EBV) Reactivation
Yale researchers found that individuals with PVS were more likely to have evidence of reactivated EBV, suggesting the vaccine may have triggered viral reactivation in susceptible individuals.
5. Autoimmune Markers
Some PVS patients show:
- Presence of autoantibodies
- Immune complexes in tissue biopsies
- Other markers of immune system dysfunction
Important caveat: These tests are not yet widely available or standardized for clinical use. They’re primarily being used in research settings. However, they confirm that PVS is a real, measurable, biological condition. It is not psychosomatic.
Specialized clinics like Leading Edge Clinic stay current on the latest diagnostic advances and can order appropriate testing when available.
Self-Assessment: Do You Have Post-Vaccine Syndrome?
Use this checklist to assess whether you may have PVS. This is not a substitute for medical diagnosis, but it can help you determine if you should seek specialized evaluation.
Post-Vaccine Syndrome Self-Assessment Checklist
You may have Post-Vaccine Syndrome if:
☐ Timeline: Your symptoms started days to weeks to months of COVID-19 vaccination
☐ Duration: Your symptoms have lasted 4 weeks or longer (many patients: months to years)
☐ No COVID: You have no evidence of COVID-19 infection (negative tests, no known exposure, no symptoms before vaccination)
☐ Multi-symptom: You have 3 or more of these core symptoms:
- Exercise intolerance / Post-exertional malaise
- Excessive, persistent fatigue
- Brain fog or cognitive issues
- Numbness, tingling, or neuropathy
- Heart palpitations or dysautonomia
- Sleep disturbances
- Multi-system symptoms (GI, muscle pain, temperature regulation)
☐ Severity: Your symptoms significantly impact your daily life, work, or ability to function
☐ No other explanation: Your doctor has ruled out other medical conditions, or you haven’t found another diagnosis that explains all your symptoms
☐ Normal tests: You’ve had normal or near-normal results on standard medical tests, but you still feel very sick
☐ No improvement: Your symptoms haven’t improved over time or with standard treatments
What Your Results Mean:
If you checked 5 or more boxes: You should strongly consider evaluation by a physician who specializes in Post-Vaccine Syndrome. Your symptom pattern and timeline are consistent with PVS.
If you checked 3-4 boxes: You may have PVS or a related condition. A thorough evaluation by a knowledgeable provider would be beneficial.
If you checked 1-2 boxes: Your symptoms may be related to other factors, but if you’re concerned, consult with a healthcare provider.
Important: This self-assessment is for informational purposes only. Only a qualified healthcare provider can diagnose Post-Vaccine Syndrome.
What to Do If You Think You Have Post-Vaccine Syndrome
If you recognize yourself in these symptoms, here are the next steps:
1. Document Your Timeline
Create a detailed record:
- Date(s) of COVID vaccination: Which vaccine (Pfizer, Moderna, J&J)? First, second, third dose?
- Symptom onset: Exactly when did symptoms start? Hours? Days? Weeks after vaccination?
- COVID testing history: Any positive tests? When? Any known exposures?
- Symptom progression: How have symptoms changed over time?
- Impact on life: How have symptoms affected work, daily activities, quality of life?
Why this matters: The temporal relationship between vaccination and symptom onset is crucial for diagnosis. A clear timeline helps your doctor understand your case.
2. Track Your Symptoms
Keep a symptom diary:
- Daily symptom severity (scale of 1-10)
- Activities that trigger or worsen symptoms
- Patterns (better or worse at certain times of day?)
- What helps or doesn’t help
3. Gather Medical Records
Collect:
- Previous test results (bloodwork, imaging, cardiac tests)
- Previous diagnoses or differential diagnoses
- Medications tried and results
- Other medical conditions or history
4. Find a Knowledgeable Provider
This is the most important step. Not all doctors are familiar with Post-Vaccine Syndrome. You need a provider who:
- Recognizes PVS as a real condition
- Has experience treating spike protein-related illness
- Uses an integrative, root-cause approach
- Stays current on the latest research
- Won’t dismiss your symptoms
Leading Edge Clinic specializes in Post-Vaccine Syndrome diagnosis and treatment. Our team has treated over 3,500 patients with spike protein-related conditions and stays at the forefront of PVS research and treatment protocols.
We offer:
- Comprehensive evaluation and diagnosis
- Evidence-based treatment protocols
- Nationwide telehealth access (all 50 states)
- Compassionate care from providers who understand PVS
- No referral required
Ready to get help? Register as a patient: https://drpierrekorypatientportal.md-hq.com/registration
5. What to Expect in Your Evaluation
When you see a PVS specialist, expect:
Comprehensive intake:
- Detailed medical history
- Timeline of symptom onset
- Review of all symptoms across body systems
- COVID and vaccination history
Appropriate testing:
- Check for biomarkers (when available)
- Assess inflammation, immune function, vitamin/nutrient levels
- Possible spike protein testing or antibody panels
Personalized treatment plan:
- Medications and supplements tailored to your symptoms
- Protocols to reduce spike protein burden
- Immune modulation strategies
- Redox repair and balancing
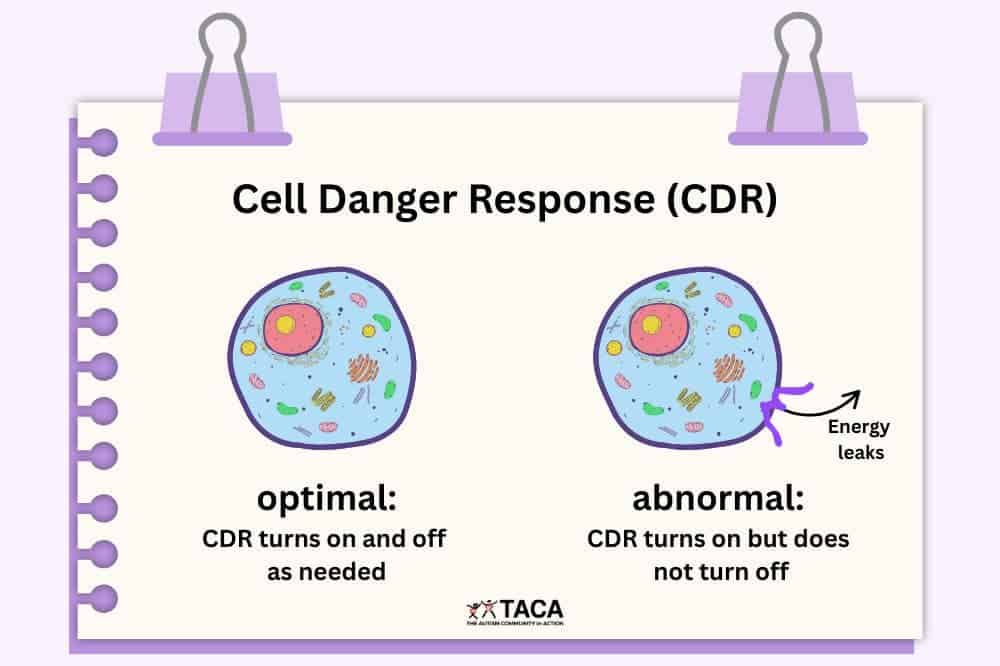
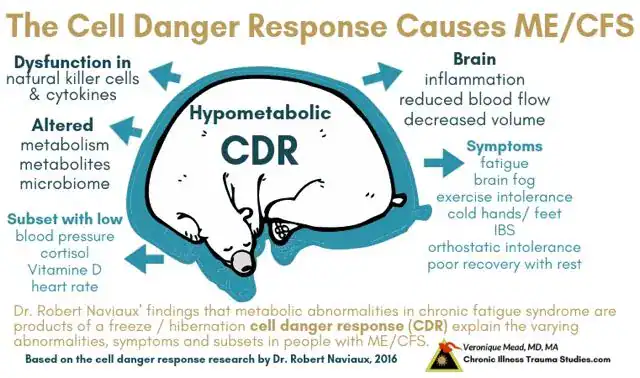
- Chornic cell danger response modulation
- Symptom management
- Lifestyle modifications
Ongoing support:
- Regular follow-ups to track progress
- Treatment adjustments based on response
- Access to nursing staff for questions
- Comprehensive, coordinated care
LINK: Learn more about our Post-Vaccine Syndrome treatment program
6. Treatment Overview: What Works for PVS?
While every patient is different, effective PVS treatment typically includes:
Spike Protein Clearance:
- Intermittent fasting (promotes autophagy)
- Specific supplements and medications shown to help clear spike protein
- Protocols to support the body’s natural detoxification and redox
Immune System Support:
- Immune-modulating agents to calm overactive immune response
- Anti-inflammatory protocols
- Treatment of viral reactivation (if present)
Symptom Management:
- Medications for dysautonomia, POTS-like symptoms
- Pain management protocols
- Sleep support
- Cognitive function support
Root Cause Approach:
- Addressing mitochondrial dysfunction and cell danger response
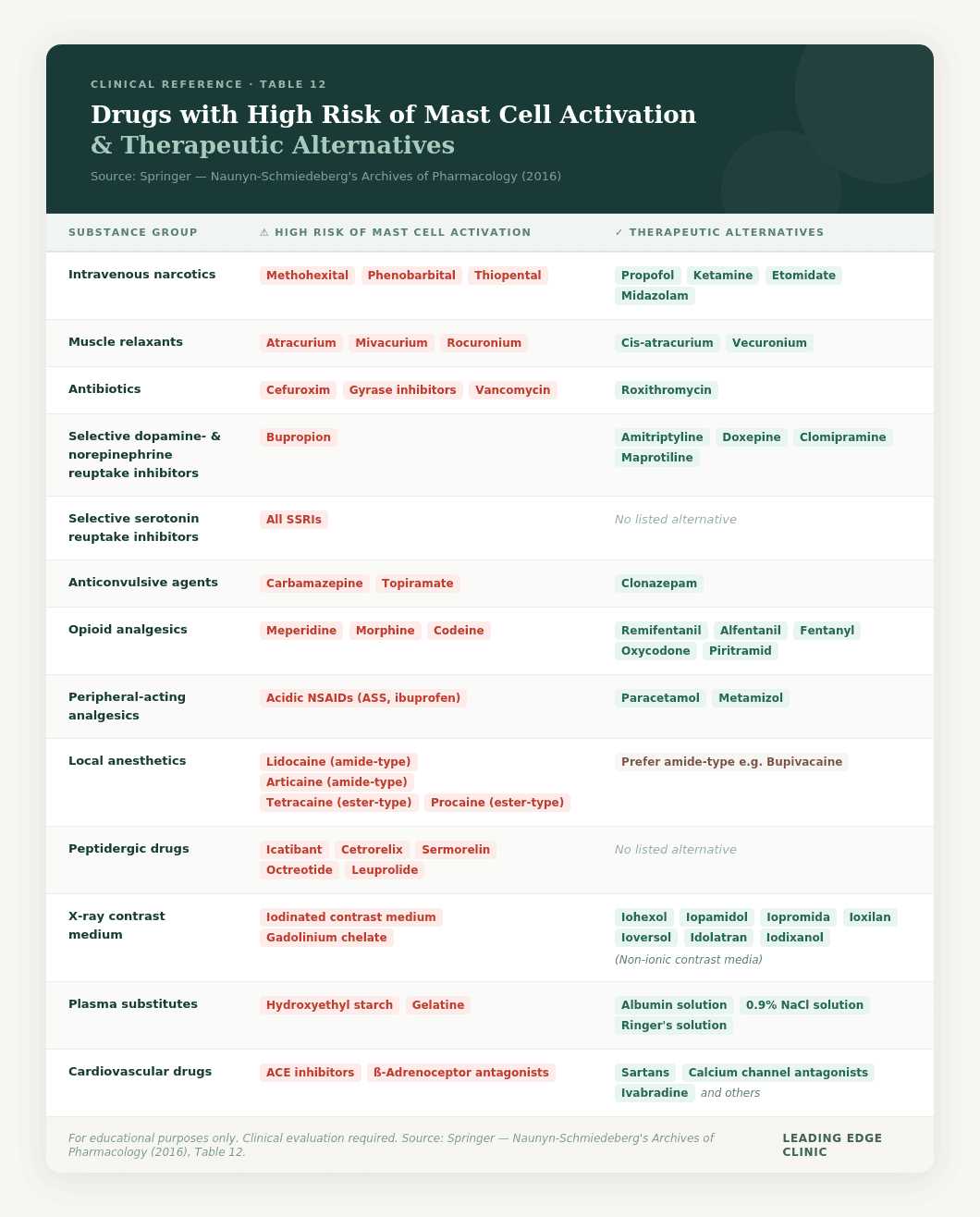
- Mast cell stabilization (if MCAS is present)
- Gut health restoration
- Micronutrient optimization
- Endothelial healing
Important: Treatment is individualized based on your specific symptoms, severity, and response. What works for one patient may need adjustment for another.
Our providers have refined treatment protocols based on thousands of patient encounters and stay current on the latest research. LINK: Meet our providers who specialize in Post-Vaccine Syndrome
The Most Important Thing to Know
If you’re reading this and recognizing yourself in these symptoms, here’s what you need to know:
1. You’re Not Alone
Even with data most likely undercounting Post-Vaccine Syndrome (affecting an estimated 0.02-2% of vaccinated individuals), that still represents potentially 500,000 to 5.4 million people in the United States alone. You are not the only one experiencing this.
2. It’s Real
Despite what some doctors may say, Post-Vaccine Syndrome is:
- Recognized by researchers at Yale, NIH, and leading medical centers worldwide
- Backed by peer-reviewed published research
- Characterized by measurable biological markers
- A somatic (physical) condition, not psychosomatic
You are not imagining this. You are not anxious or depressed (or if you are, it’s because of the physical illness, not the cause). Your symptoms are real.
3. You’re Not Being Hysterical
Acknowledging that you’ve been injured by a vaccine doesn’t make you crazy. It makes you honest about your experience.
You deserve medical care regardless of the political implications of your diagnosis.
4. Treatment Is Available
Post-Vaccine Syndrome is treatable. While recovery takes time, and there’s no “quick fix,” many patients see significant improvement with:
- Proper diagnosis and recognition of the condition
- Evidence-based treatment protocols targeting spike protein clearance and immune modulation
- Comprehensive symptom management
- Supportive care from knowledgeable providers
5. Early Recognition Leads to Better Outcomes
The sooner you receive proper diagnosis and treatment, the better your chances of recovery. Don’t wait months or years suffering while doctors tell you “nothing is wrong” or that you need antidepressants.
If you recognize the warning signs, seek specialized care now.
6. You Deserve to Be Believed
Too many PVS patients have been dismissed, gaslit, or told their symptoms are psychosomatic. You deserve a doctor who:
- Listens to you
- Believes your symptoms are real
- Takes your suffering seriously
- Works with you to find solutions
At Leading Edge Clinic, we see you, we believe you, and we’re here to help.
Take the Next Step
If you’ve recognized yourself in these seven warning signs, don’t wait. Post-Vaccine Syndrome doesn’t improve on its own. It requires specialized diagnosis and treatment.
What you can do right now:
- Download our symptom tracker to start documenting your symptoms (COMING SOON)
- Read our FAQs about Post-Vaccine Syndrome diagnosis and treatment
- Register as a patient at Leading Edge Clinic—no referral required – https://drpierrekorypatientportal.md-hq.com/registration
- Watch patient testimonial videos from others who have recovered from PVS with our help
- Learn about our providers who specialize in spike protein-related illness:
Frequently Asked Questions
Q: How long do Post-Vaccine Syndrome symptoms last?
A: Without treatment, symptoms can persist for months or years, and increase in severity. The median duration in the Yale LISTEN Study was nearly 20 months, and many patients had symptoms lasting even longer. With proper treatment, many patients see improvement, though recovery timelines vary.
Q: Can Post-Vaccine Syndrome be cured?
A: While “cure” isn’t the right word for a complex multi-system condition, many patients experience significant recovery with proper treatment. The goal is to reduce spike protein burden, modulate the immune system, and support the body’s natural healing. Many patients return to normal or near-normal functioning.
Q: Will I need to see a doctor in person?
A: No! Leading Edge Clinic offers comprehensive telehealth services to patients in all 50 states. All consultations and follow-ups can be done virtually via secure video appointments.
Q: Does insurance cover Post-Vaccine Syndrome treatment?
A: We do not participate in insurance. Some patients submit their appointment costs to their insurance providers after the fact to try and get reimubrsement. Coverage varies by insurance plan. We recommend checking with your insurance provider. Many of our patients use HSA/FSA funds for treatment costs. We partner with Opus Health for this
Q: What if I’ve already seen multiple doctors who say nothing is wrong?
A: This is extremely common with PVS patients. Standard medical tests often come back normal or show only minor abnormalities, leading many doctors to conclude you’re fine when you clearly aren’t. Specialized providers who understand PVS know how to recognize the condition even when standard tests are normal and know what testing to order to identify biomarkers and guide treatment.
Q: Can I have both Long COVID and Post-Vaccine Syndrome?
A: Yes, it’s possible to have overlapping conditions, especially if you had COVID and then were vaccinated while still experiencing symptoms. A detailed timeline helps clarify the primary driver of your symptoms. But, more importantly, treatment will be extremely similar, if not identical.
About Leading Edge Clinic
Leading Edge Clinic specializes in complex, multi-system illnesses including Post-Vaccine Syndrome, Long COVID, MCAS, and other spike protein-related conditions. Founded by Dr. Pierre Kory and Scott Marsland, FNP-C, we’ve treated over 3,500 patients nationwide using evidence-based protocols and a compassionate, patient-centered approach.
Our team includes physicians and nurse practitioners who are experts in:
- Post-Vaccine Syndrome diagnosis and treatment
- Spike protein pathology and clearance protocols
- Long COVID and post-viral illness
- MCAS and immune dysregulation
- Complex chronic conditions
- Adjunctive Cancer Care with repurposed drugs
We offer telehealth appointments to patients in all 50 states, making specialized care accessible no matter where you live.
Learn more about our approach – https://drpierrekory.com/why-leading-edge-clinic/
Resources and Further Reading
Research on Post-Vaccine Syndrome:
- Yale LISTEN Study: Post-Vaccination Syndrome: A Descriptive Analysis
- Immune markers of post-vaccination syndrome: Yale News
- Chronic Fatigue and Dysautonomia following COVID-19 Vaccination: PMC Study
Related Blog Posts:
- Long Covid vs Post-Vaccine Syndrome: What’s the Difference?
- MCAS and Long Covid: The Connection & Treatment Options
- The Cell Danger Response
Get Help:
Disclaimer: This article is for informational purposes only and is not intended to diagnose, treat, cure, or prevent any disease. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Published: March 2026 Author: Leading Edge Clinic Medical Team
If you found this guide helpful, please share it with others who may be experiencing Post-Vaccine Syndrome symptoms. Early recognition and treatment can make a significant difference in recovery.