Why Everything You’ve Been Told About Cancer May Be Wrong — And What the Science Actually Shows
Introduction: The Theory That Has Cost Millions of Lives
In 1971, President Nixon declared a “War on Cancer.” The United States has spent hundreds of billions of dollars on cancer research since. The result, by any honest accounting, has been deeply disappointing.
Deaths from cancer have increased 9% since 1950. The overall contribution of chemotherapy to five-year survival in adults is estimated at roughly 2% in the United States. Over the past fifteen years, new cancer therapies have improved overall survival by an average of 2.4 months. Over the past thirty years, all advances in experimental treatment have yielded a collective improvement of 3.4 months in overall survival.
These are the numbers of a field that has been looking in the wrong place for a very long time.
In this case, the wrong place is the nucleus. And the incorrect framework is the Somatic Mutation Theory of cancer, which is the consensus model that has guided oncology research and treatment for over 70 years. Evidence that overturned it has been sitting in the scientific literature for fifteen years, largely ignored by the institutions that fund cancer research and the oncologists who treat patients.
At Leading Edge Clinic, we have built a complementary cancer care program around the framework that replaced it: the Metabolic Theory of Cancer. This post explains what that theory is, why the evidence supports it, and what it means for how cancer should be treated, including the role of repurposed drugs and metabolic interventions that most oncologists are still not discussing with their patients.
Two Theories of Cancer: A Fundamental Disagreement
To understand why the Metabolic Theory of Cancer matters, you first need to understand what it is competing against.
The Somatic Mutation Theory (SMT) holds that cancer arises from the accumulation of genetic mutations in the DNA contained within the nucleus of a cell. Carcinogens damage genes, specifically tumor suppressor genes and tumor promoter genes, and these mutations drive the cell to acquire the eight hallmarks of cancer identified by Hanahan and Weinberg: uncontrolled growth, evasion of cell death, immune evasion, the ability to spread, and critically, a reprogramming of energy metabolism.
The SMT has been the foundational, total, and guiding theory of cancer since the early 1970s. It is the basis for the entire field of “targeted therapy” drugs designed to counteract the products of specific genetic mutations.
The Metabolic Theory of Cancer (MTOC) holds something fundamentally different. It posits that cancer begins not with nuclear DNA damage but with damage to the mitochondria, the energy-producing organelles in the cell’s cytoplasm. When mitochondria are damaged, they lose the ability to use oxygen for energy production and are forced instead to rely almost entirely on glucose fermentation. This metabolic switch is known as the Warburg Effect, and was first identified by Nobel laureate Otto Warburg in 1927. This switch is then what sends distress signals to the nucleus, disrupting DNA repair mechanisms and activating oncogenes. Under the MTOC, nuclear mutations are a consequence of mitochondrial dysfunction, not its cause.
With this distinction, comes a fundamental difference in what you treat, how you treat it, and with what.

The Failure of the Somatic Mutation Theory
The SMT ran into serious trouble the moment large-scale genomic sequencing became possible.
The Cancer Genome Atlas Project
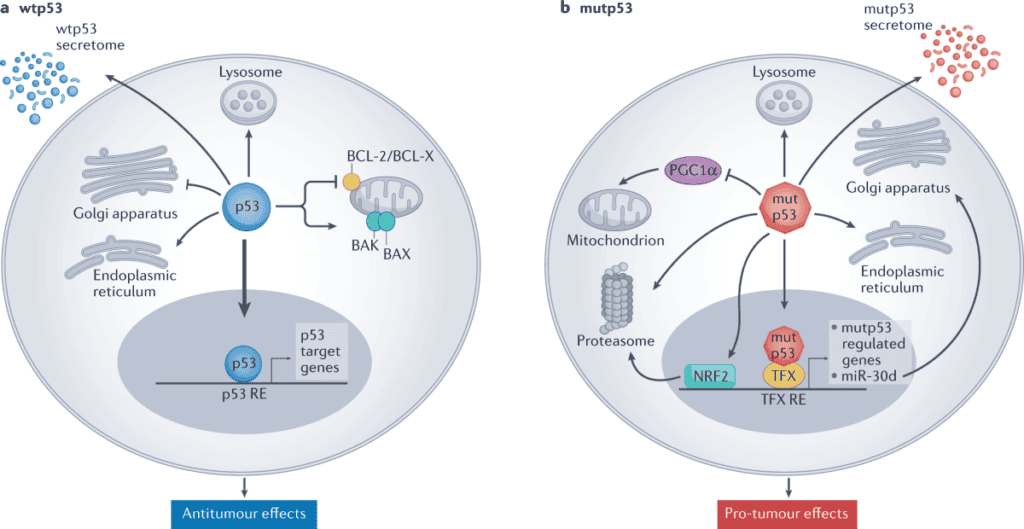
In 2005, the Cancer Genome Atlas Project (TCGA) was launched. It was a massive, well-funded effort to sequence the genomes of cancer cells across multiple cancer types. The goal was to identify the mutations driving cancer, providing the targets for the next generation of therapies. Vogelstein, the most prominent SMT researcher of his era and the scientist who found that p53 mutations occur in more than 50% of cancers, was centrally involved.
What the TCGA found was not confirmation of the SMT. It was its systematic dismantling.
Across tumor types, the project found random mutations throughout the genome — no orderly progression of successive mutations as the theory predicted. Few previously unknown oncogenes were identified. No single “founding mutation” — a mutation that would need to be present in every cancer cell if the SMT were correct — was found. Mutations differed dramatically between patients with the same cancer type. Even within a single patient’s tumor, mutations varied widely between cells. In breast cancer, five tumors had no mutations at all while still behaving aggressively and cancerously.
The last finding is particularly damning. If nuclear mutations cause cancer, then every cancer cell, being a daughter of the original mutated cell, must carry that founding mutation. If you find cancer cells without any founding mutation, the Somatic Mutation Theory is dead. No founding mutation has been found to date.
In response, Vogelstein repeatedly modified the SMT to accommodate the contradictory data, eventually proposing twelve distinct biological systems that cancer could disrupt, which Travis Christofferson in his book Tripping Over the Truth described as “an ad hoc modification necessary to make a failed theory fit the data.” He eventually abandoned the study of cancer causes entirely, shifting his focus to diagnostics.
The field of targeted therapies (seven hundred agents tested in solid tumor patients over the past decade) produced zero drugs that prolonged survival by one year compared to conventional treatment. Zero. This is what you get when you design drugs against targets that are consequences rather than causes.
The Metabolic Theory: What Warburg Found and Why It Was Ignored
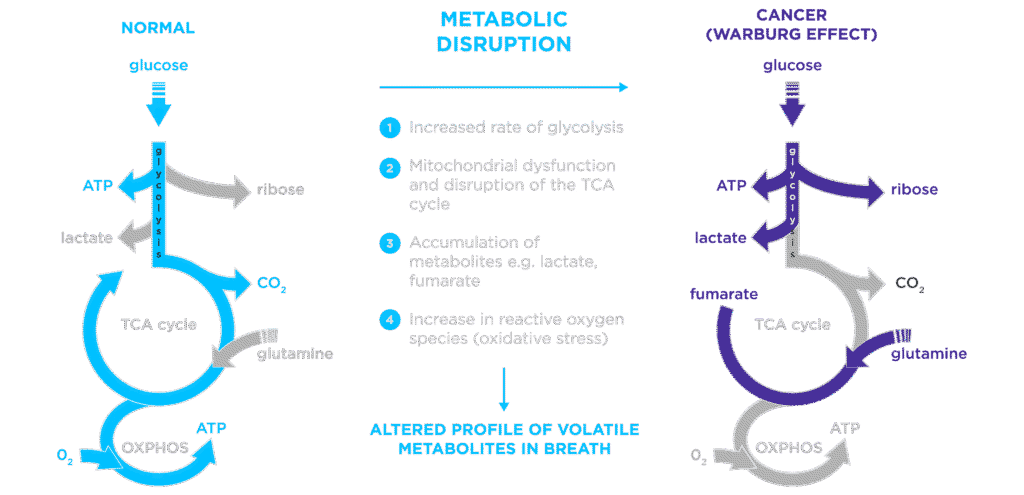
Otto Warburg discovered in 1927 that cancer cells, unlike normal cells, rely almost exclusively on glucose fermentation for energy, even in the presence of oxygen. He spent the rest of his life arguing this was not a curiosity but the central defining feature of a cancer cell. He won the Nobel Prize in 1931 for this discovery.
The Warburg Effect is, notably, the biological basis of PET scanning, which are the imaging technology that every oncologist uses to diagnose, stage, and monitor cancer. PET scans inject radio-labeled glucose into patients and identify cancer by the areas of unusually high glucose uptake. Every oncologist who orders a PET scan is implicitly acknowledging the Warburg Effect, that cancer cells are defined by their glucose dependence, while simultaneously telling patients that diet has no bearing on their cancer.
The question Warburg could never answer in his lifetime was why. Why do cancer cells rely on glucose even when oxygen is available?
Pedersen, Seyfried, and the Nuclear Transfer Experiments
The answer came from decades of work by Pete Pedersen, beginning in 1979, and was assembled into a coherent theory by Dr. Thomas Seyfried at Boston College in the early 2000s.
Pedersen discovered that cancer cells had structurally abnormal mitochondria. There were fewer of them, they were smaller, and they had missing membranes and abnormal protein content. He found that cancer cells expressed a specific, overactive form of hexokinase that both drove glucose consumption to its maximum and simultaneously inhibited apoptosis (programmed cell death). He established that carcinogens which better damaged mitochondria were better at causing cancer than those which damaged chromosomes.
Seyfried assembled these findings into a complete theory, grounded in nuclear transfer experiments from the 1980s that had been performed and then effectively ignored.
In these experiments, researchers took the nucleus of a cancer cell and transferred it into a normal cell from which the nucleus had been removed. If cancer was caused by nuclear mutations — as the SMT held — these reconstituted cells should have behaved cancerously. Instead, in study after study, they did not. The healthy mitochondria in the host cell appeared to silence the cancerous nuclear DNA.
The reverse experiment was equally decisive. When mitochondria from a cancer cell were transferred into a normal cell with a healthy nucleus, 97% of the resulting mice developed cancer.
The conclusion was unambiguous: damaged mitochondria, not mutated nuclei, are the proximate cause of cancer. The mutations found in cancer nuclei are downstream consequences of mitochondrial dysfunction, not its upstream cause.
Seyfried published his synthesis in 2012 in his book Cancer as a Metabolic Disease. He received standing ovations at medical conferences. The National Cancer Institute declined to meaningfully shift its research funding priorities.
How the Two Theories Fit Together
It’s important to be precise here, because the MTOC does not deny that nuclear mutations exist in cancer — they clearly do. What it argues is that these mutations are not the primary driver. They are consequences of mitochondrial dysfunction.
Damaged mitochondria send signals back to the nucleus (what Seyfried called the “retrograde response”) that disrupt DNA repair mechanisms and activate oncogenes. The mutations observed in cancer cells arise because the cellular machinery for monitoring and correcting DNA errors has been compromised by the initial mitochondrial insult.
This means that the SMT is not entirely wrong. It is, as Seyfried has argued, incomplete. The mutations are real. They are just not the starting point. And designing cancer therapy exclusively around targeting those mutations,while ignoring the metabolic dysfunction that generated them, is precisely why targeted therapy has delivered such modest results.
The two theories can and should coexist in clinical practice. At Leading Edge Clinic, we do not advise patients to forego standard of care. We argue that standard of care should be complemented with metabolic interventions, because if metabolic dysfunction is primary, then metabolic intervention must be part of the treatment.
The Warburg Effect and the Ketogenic Diet
The most immediate clinical implication of the MTOC is dietary.
If cancer cells are defined by their dependence on glucose, and if normal cells can switch to burning ketone bodies derived from fat when glucose is unavailable (while cancer cells generally cannot, because this requires functional mitochondria) then a ketogenic diet creates a metabolic environment that selectively disadvantages cancer cells while supporting normal ones.
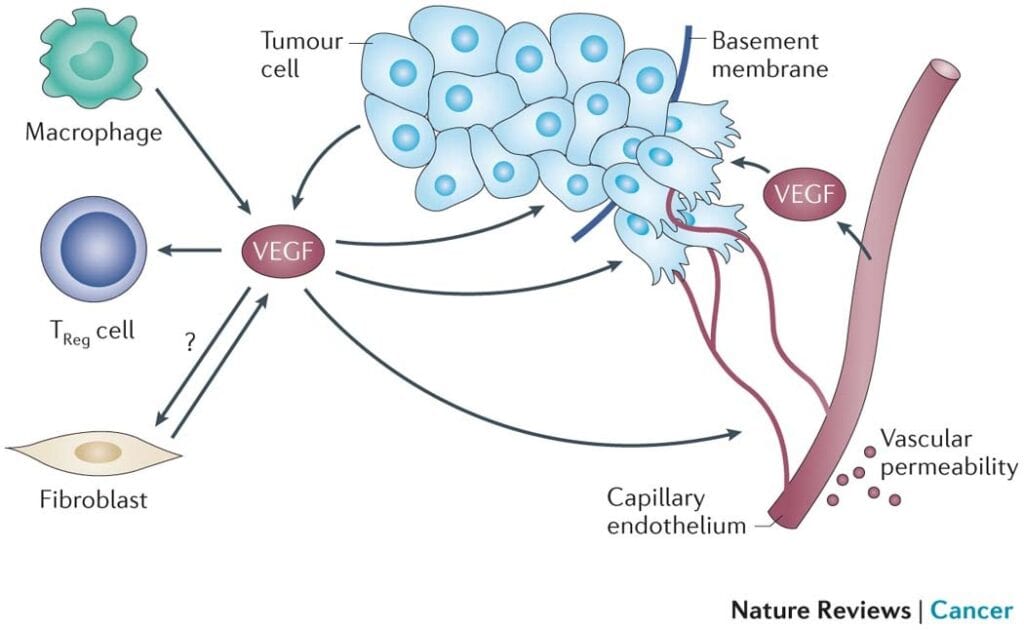
Thomas Seyfried tested this in animal models and found that caloric restriction and ketogenic diets were anti-angiogenic, pro-apoptotic, anti-invasive, and restored normal aerobic metabolism. This pushes back on nearly every mechanism by which cancer cells sustain their cancerous behavior.
Published studies support beneficial impacts of ketogenic and caloric restriction approaches across multiple cancer types including breast, brain, colon, pancreas, lung, and prostate cancers. Studies also show that such dietary approaches reduce chemotherapy side effects and potentiate chemotherapy efficacy. Patients who combine ketogenic diet with radiation or chemotherapy appear to do better than with either alone.
When we ask our cancer patients what their oncologist told them about nutrition, the most common answer is: “whatever you like.” A PET scan that lights up because of glucose uptake, ordered by a clinician who tells their patient diet doesn’t matter, represents a profound disconnection between the diagnostic tool and the treatment philosophy.

Repurposed Drugs: The Clinical Application of the MTOC
Metabolic dysfunction in cancer cells creates multiple therapeutic vulnerabilities that can be targeted by drugs already in clinical use for other indications. This is the foundation of the repurposed drug approach to cancer.
Dr. Paul Marik, co-founder of the FLCCC and Dr. Kory’s longtime colleague, conducted a comprehensive scoping review of nearly 1,500 scientific references on repurposed drugs and nutraceuticals in cancer treatment, compiled in his book Cancer Care. He graded the evidence for each compound, identifying seventeen with strong evidence, eight with weak evidence, and fifteen with insufficient evidence.
At Leading Edge Clinic, we work from the compounds with both strong published evidence bases, but also the backing of our own clinical experiences. The result is combinations of agents depending on cancer type and stage. The pathways we target with repurposed drug combinations include Hexokinase 2, p53, TGF-β, Wnt, Notch, PI3K/AKT, Hedgehog, IGF-1, and more. These are all metabolic or growth-signaling pathways that are disrupted in cancer cells.
What the Clinical Trials Show
The repurposed drug approach is not speculative. A growing body of clinical trial evidence, primarily from academic centers outside the United States, where practitioners are less financially constrained to standard of care, shows meaningful results.
CUSP9 (glioblastoma): Nine repurposed drugs added to standard of care. Phase 1 trial results: 30% of patients alive and disease-free at over four years post-treatment. Historical standard of care long-term survival: under 5–10%.
METRICS (glioblastoma): Four repurposed drugs — metformin, atorvastatin, mebendazole, and doxycycline — added to standard of care in 95 Stage IV patients. Two-year survival: 64% versus 26–28% in historical controls. Median survival: 27.1 months versus 14–15 months. 85% of patients tolerated all four drugs without difficulty.
CLOVA (glioblastoma): Four different repurposed drugs — cimetidine, lithium, olanzapine, and valproate — in seven patients with recurrent, chemotherapy-resistant GBM with the poorest predicted prognosis. Median overall survival after recurrence: 11.2 months versus 4.3–4.9 months in historical controls (p=0.004).
COMBAT (pediatric solid tumors): Celecoxib, vitamin D, fenofibrate, and retinoic acid alongside standard chemotherapy in 74 children with advanced, heavily pretreated tumors. In the high-grade sarcoma subgroup: median overall survival of 15.4 months versus 3.9 months in historical controls — nearly four times longer (p=0.001).
These are meaningful, consistent improvements in survival across multiple cancer types, in multiple independent research groups, with multiple different drug combinations. What they all share in common is the thread of targeting metabolic and growth pathways rather than specific genetic mutations.
The ReDO (Repurposing Drugs in Oncology) Project, a partnership between The AntiCancer Fund and Global Cures, has now identified 970 trials of repurposed drugs in cancer across 45 countries. There is real momentum and there are reall results behind this approach. The barrier to widespread scientific inquiry is primarily financial. Repurposed drugs are off-patent, so there is no commercial incentive to fund large trials, and pharmaceutical companies are not funding the research that would establish their efficacy.

Cancer Stem Cells: The Target Standard Therapy Misses
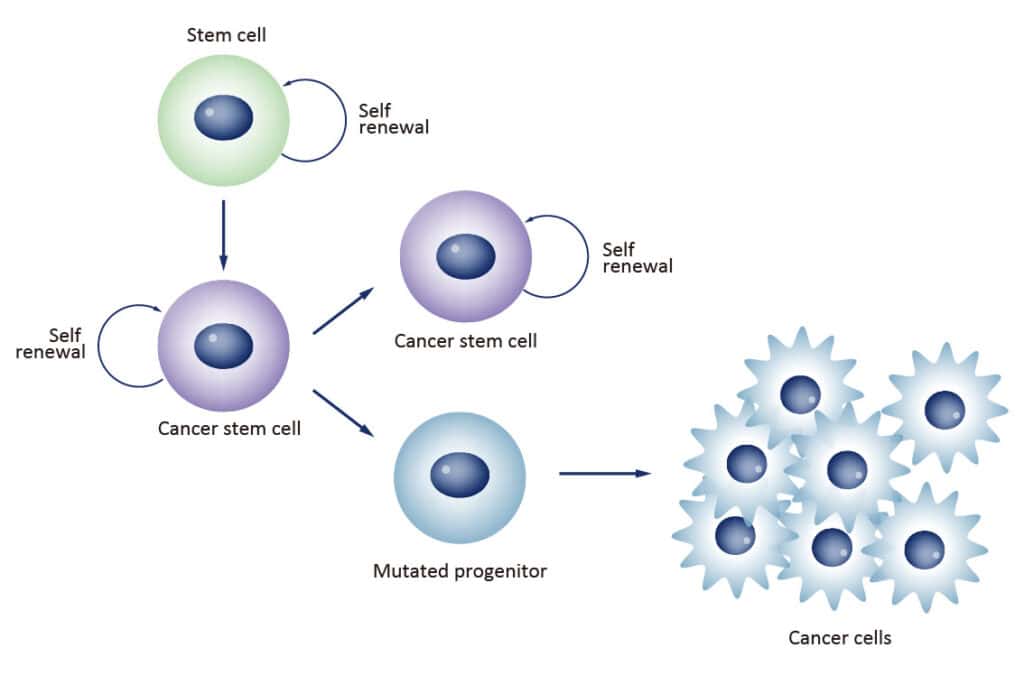
One of the most important, and most overlooked, aspects of why standard cancer therapies so often fail is the cancer stem cell problem.
Cancer stem cells (CSCs) are a small, resilient subset of tumor cells (comprising between 0.01% and 2% of a tumor) that drive growth, relapse, and metastasis. Unlike the rapidly dividing cancer cells that chemotherapy and radiation target, CSCs exhibit self-renewal, differentiation, and anti-apoptotic properties that make them resistant to conventional treatment.
More troublingly, there is published evidence that chemotherapy and radiation can actively promote CSC proliferation, meaning the treatments that shrink tumors can simultaneously stimulate the very cells most responsible for recurrence. There are currently no FDA-approved therapies specifically targeting cancer stem cells.
Repurposed drugs change this picture. Since the discovery of CSCs, extensive in vitro studies have identified affordable, accessible agents that inhibit CSC proliferation. At Leading Edge Clinic, we specifically target CSCs in our combination protocols, which may include agents such as metformin, ivermectin, mebendazole, doxycycline, curcumin, green tea extract, berberine, melatonin, statins, and vitamin D3. Of course, the combinations used are specific to individual patients, and this is not an exhausitve list.
Targeting cancer stem cells is a response to one of the most important reasons that standard therapies produce high initial response rates followed by relapse. If you shrink the tumor while stimulating the cells that will rebuild it, you have not solved the problem.
Our Approach at Leading Edge Clinic
Our position is explicit: we do not recommend that patients avoid standard of care oncology. What we offer is a complement to that care, a metabolic and repurposed drug framework layered alongside standard treatment, aimed at the mechanisms that standard treatment leaves unaddressed.
Our approach may include some combination of:
Metabolic intervention. Ketogenic and caloric restriction dietary protocols, individualized to the patient’s cancer type, treatment status, and physical condition. The Warburg Effect is real. A clinical approach that ignores dietary glucose is ignoring the biology.
Repurposed drug combinations. Drawn from the strongest evidence base, targeting multiple growth-driving pathways simultaneously. We do not use single agents. The evidence strongly favors combination approaches, which is why CUSP9, METRICS, and CLOVA used four to nine agents at once.
Cancer stem cell targeting. Specific agents selected for anti-CSC mechanisms, addressing the relapse problem that standard therapy systematically fails to address.
Observational study enrollment. Leading Edge Clinic is a study site for a prospective, IRB-approved observational study comparing outcomes in patients treated with complementary repurposed drug protocols versus standard of care alone. It is being conducted through the nonprofit Rebuild Medicine. This is the scientific infrastructure needed to generate the evidence that the field’s financial dynamics have prevented from being produced.
A Note on Realistic Expectations
What is this approach? What is it not?
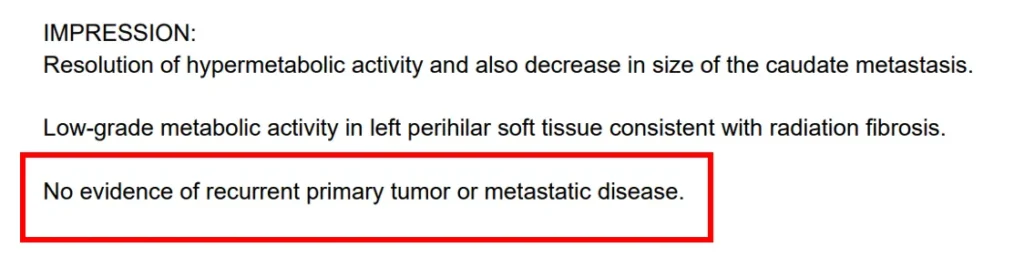
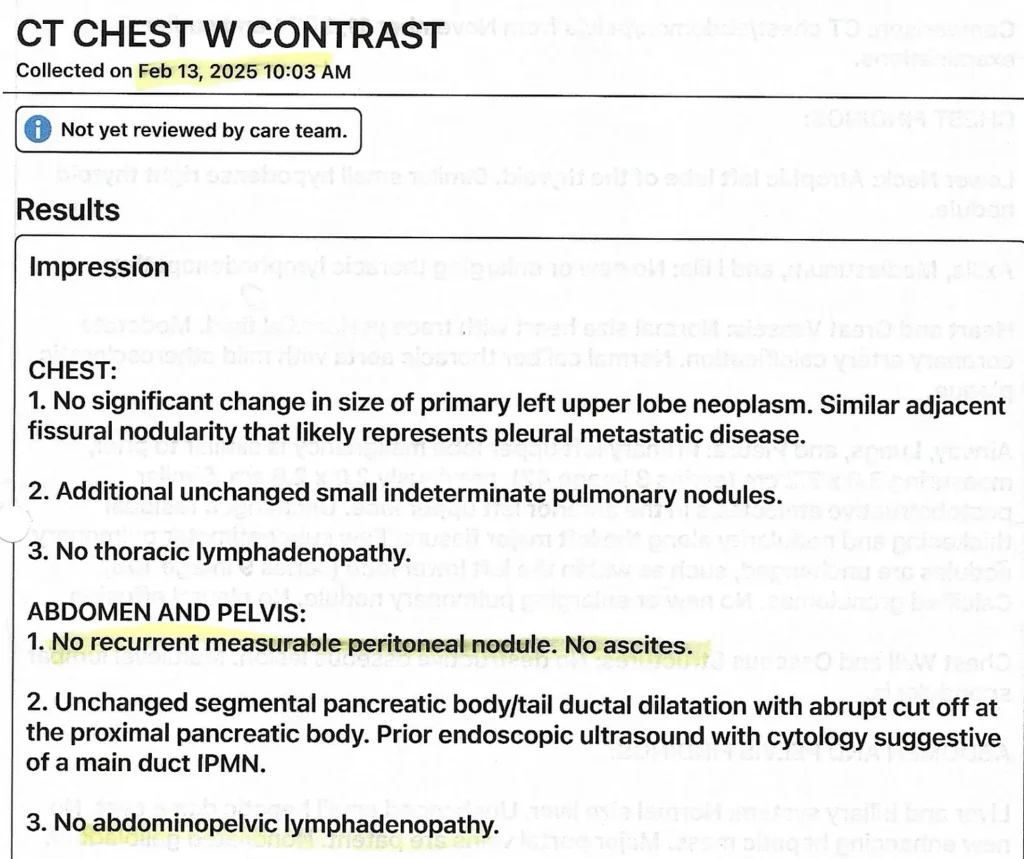
The patients who respond most dramatically to repurposed drug and metabolic protocols are not a representative sample. Dramatic responses exist. Complete and near-complete resolution of metastatic disease exists, as documented in our own patient series. But, so do more modest responses, such as moderate shrinkage of tumors, or halting of disease progression. There are also, of course, patients who do not respond the way we are hoping they will. Welcome to cancer care. It is a moving target, and our approaches evolve with both our clinical experience, and emerging evidence.
We present our outcomes consecutively and transparently, not cherry-picked successes like some others in the space. Of five consecutive metastatic lung cancer patients treated at our clinic with combination repurposed drug protocols and ketogenic diets, four showed no cancer progression over the observation period. One achieved complete remission. Two of those patients (by their own choice, not our recommendation) received no conventional chemotherapy, radiation, or targeted therapies. These are meaningful results, and they should be interpreted in the context of what we know from the clinical trials above.
They are also preliminary. This is why the observational study matters. We need the data. We need to understand who responds and why, so that the clinical approach can be refined and the patients who are most likely to benefit can be identified.
What we can say with confidence is that the metabolic framework is scientifically sound, the repurposed drug evidence base is real and growing, and the gap between what standard oncology offers and what is available to patients willing to go further is substantial.
If you want to learn more about becoming a patient with our clinic, please use the following resources:
- Why Leading Edge Clinic?
- About Adjunctive Cancer Care Program
- About the Repurposed Drug Study
- A Deep Dive on Ivermectin
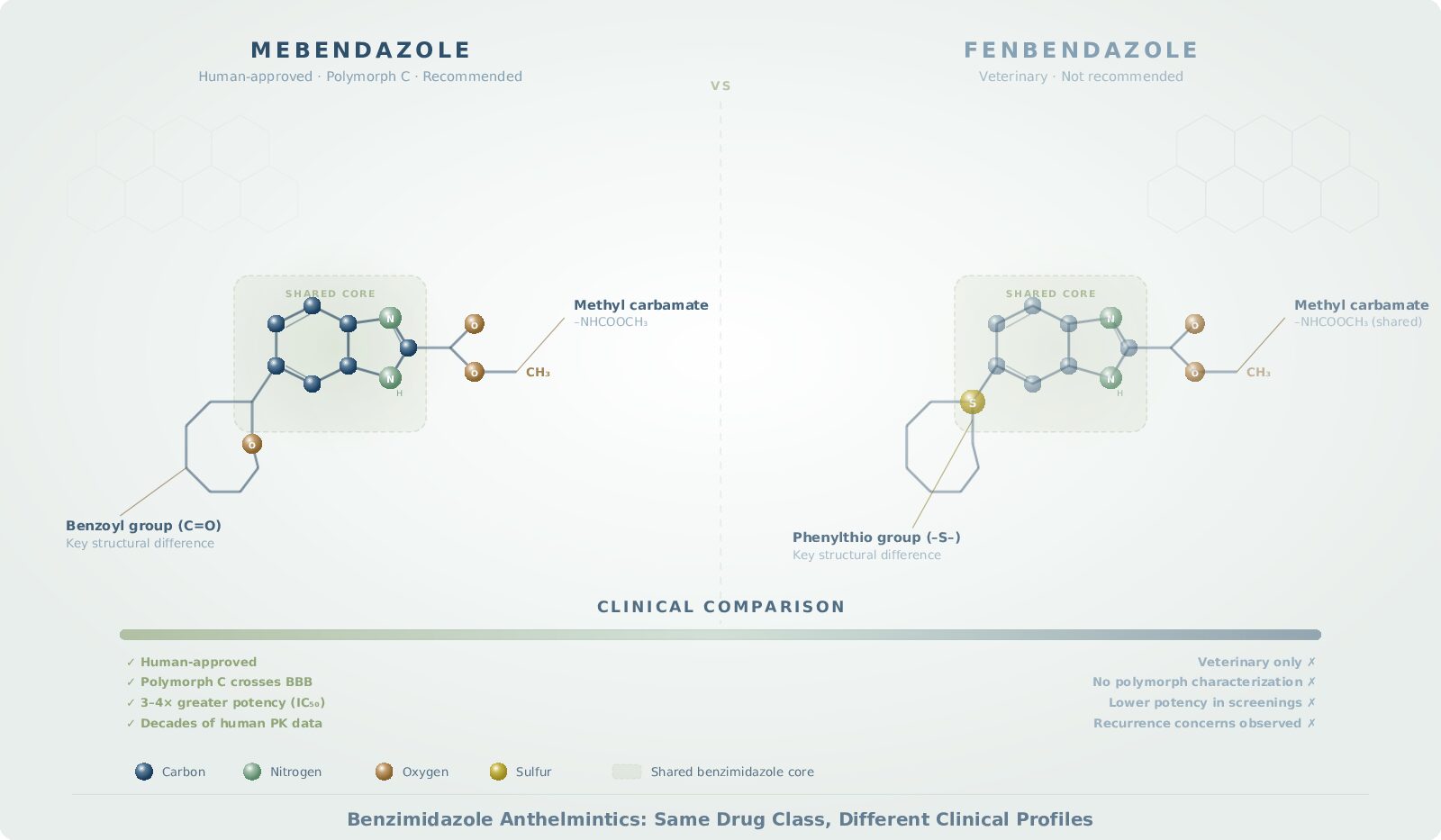
- Mebendazole vs. Fenbendazole
- Patient Interview: Multiple Myeloma
- Stage 4 Metastatic Lung Cancer Case Series – 5 patients
Leading Edge Clinic offers adjunctive cancer care alongside standard oncology, including repurposed drug protocols and metabolic interventions. We see cancer patients in all 50 states via telehealth. Leading Edge Clinic is a study site for the Rebuild Medicine observational study on repurposed drugs in cancer.
This article is for educational purposes and does not constitute medical advice. We strongly encourage all cancer patients to seek professional care for treatment.
Key References
- Seyfried TN. Cancer as a Metabolic Disease: On the Origin, Management, and Prevention of Cancer. Wiley; 2012.
- Christofferson T. Tripping Over the Truth: How the Metabolic Theory of Cancer Is Overturning One of Medicine’s Most Entrenched Paradigms. Chelsea Green; 2017.
- Marik PE. Cancer Care: The Role of Repurposed Drugs and Metabolic Interventions. 2nd ed. 2024.
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. https://doi.org/10.1016/j.cell.2011.02.013
- Warburg O. On the origin of cancer cells. Science. 1956;123(3191):309–314.
- CUSP9 trial: https://pmc.ncbi.nlm.nih.gov/articles/PMC8349180/
- METRICS trial: https://pmc.ncbi.nlm.nih.gov/articles/PMC6610246/
- CLOVA trial: https://pmc.ncbi.nlm.nih.gov/articles/PMC5410264/
- COMBAT trial: https://karger.com/ocl/article-abstract/82/5/249/327319/
- ReDO Project: http://www.redo-project.org/
- Kory P. The Scientific Basis For The Somatic Mutation Theory Is Invalid. Substack. August 2024. https://pierrekorymedicalmusings.com/p/the-scientific-basis-for-the-somatic
- Kory P. The Evolution And Validation Of The Metabolic Theory Of Cancer. Substack. November 2024. https://pierrekorymedicalmusings.com/p/the-evolution-and-validation-of-the
- Kory P. Repurposed Drugs in Oncology: Current State Of The Evidence And A Case Series In Metastatic Lung Cancer. Substack. August 2025. https://pierrekorymedicalmusings.com/p/repurposed-drugs-in-oncology-current
- Rebuild Medicine cancer observational study: https://drpierrekory.com/cancer-care-study