You went to your primary care doctor. They ran the standard panels, found nothing, and told you to rest. You pushed. Through endless research and self-advocacy, you found a Long COVID clinic – maybe a university program, maybe a telehealth practice, maybe an integrative specialist someone in your online support group recommended. You spent a significant amount of money on testing and extensive protocols, waiting to get better.
You’re still sick.
If that describes your experience, this post is for you. Our goal is to honestly explain something that most Long COVID and Post-Vaccine Syndrome clinicians — even well-meaning, intelligent ones — fundamentally misunderstand about this condition.
At Leading Edge Clinic, we’ve treated more than 3,500 patients with Long COVID and Post-Vaccine Syndrome. Many of them came to us after failing at other practices, sometimes after spending $30,000 to $100,000 elsewhere. What we’ve observed over years of clinical work has shaped a different understanding of why standard approaches so often fall short.
The Core Problem: Long COVID Is Not One Disease
The most common clinical mistake we see, across conventional medicine, integrative medicine, and Long COVID specialty practices alike, is treating this condition as if it has a singular mechanism that responds to a singular approach (ie: dealing only with spike persistence, dealing only with immune dysfunction, looking only at gut health, etc…)
It doesn’t.
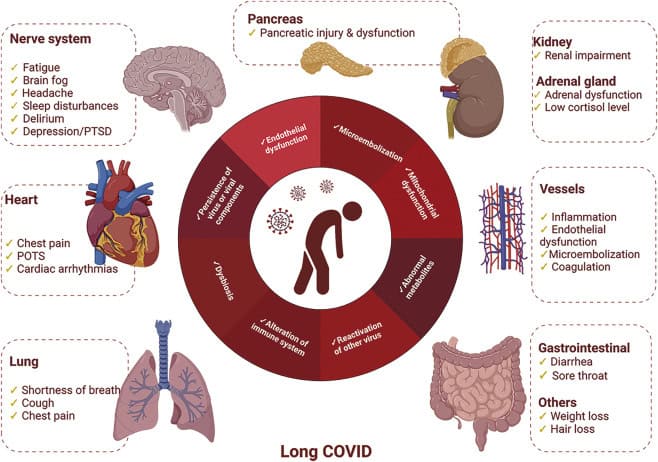
Long COVID and Post-Vaccine Syndrome are multi-system, multi-mechanism conditions that present differently in every patient and evolve over time. What’s driving your fatigue may not be the same as what’s driving the next patient’s. And critically, what’s driving your symptoms today may not be what’s driving them six months from now.
Like other historicaly post-viral and post-vaccine syndromes, this not a simple infection with a clean recovery arc. It is a dysregulated biological state, and it is very effcient at driving that dysregulated state — often involving the immune system, the nervous system, the vascular system, and the metabolic system simultaneously, in proportions that vary person to person and shift in response to treatment.
A clinician who approaches it with a fixed protocol, even a sophisticated one, is going to miss the mark for a significant portion of patients.
What Standard Approaches Miss
This is not an exhaustive list. It hits on some major systemic issues we don’t see others talking about, but these aren’t the only things we see other clinicians missing when a new patient comes to us that has tried elsewhere first.
1. They Don’t Account for Cell Danger Response
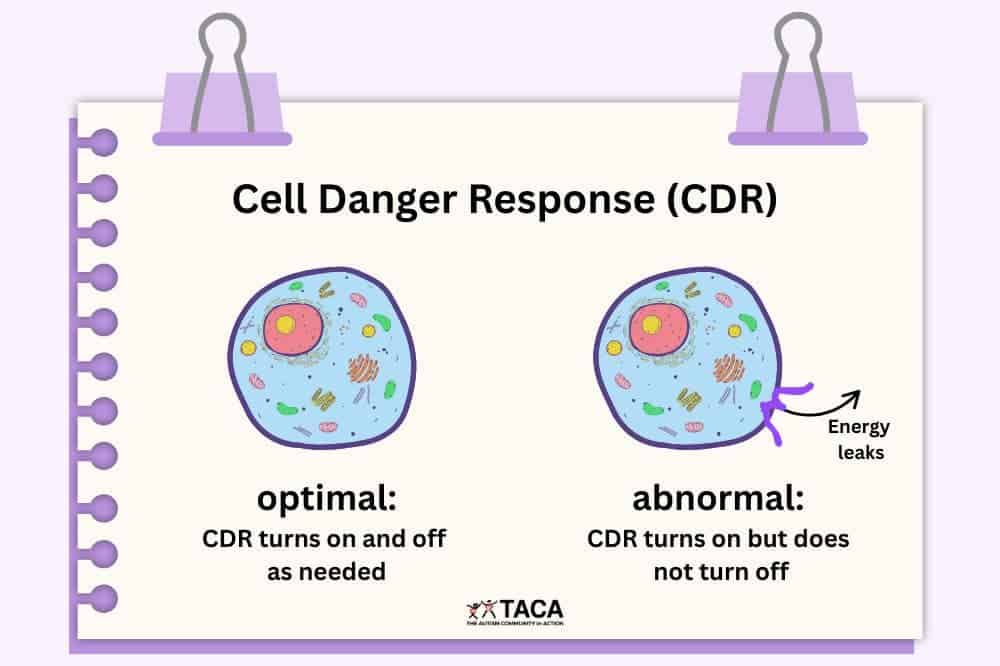
One of the most underappreciated mechanisms in Long COVID is something called the Cell Danger Response (CDR) — a concept developed by metabolic researcher Dr. Robert Naviaux.
The CDR is the body’s ancient, conserved response to threat. When cells detect danger, such as infection, toxin, or injury, they shift into a defensive metabolic state. Energy production is reduced, cellular communication slows down , and cells essentially go quiet to protect themselves.
This is adaptive in the short term. After an acute COVID infection, you want this response. It’s doing its job.
The problem is when the CDR doesn’t turn off. When the body’s threat detection system remains activated long after the initial danger has passed, you get persistent metabolic suppression. This manifests as fatigue that doesn’t resolve with rest, cognitive dysfunction that doesn’t respond to sleep, and a nervous system that stays in a low-grade defensive posture.
Most Long COVID clinicians are not testing for or thinking about CDR biology. Many deal with chronic inflammation and persistent spike protein, but never take that next step to address chronic CDR.
2. They Don’t Understand Senescent Cells
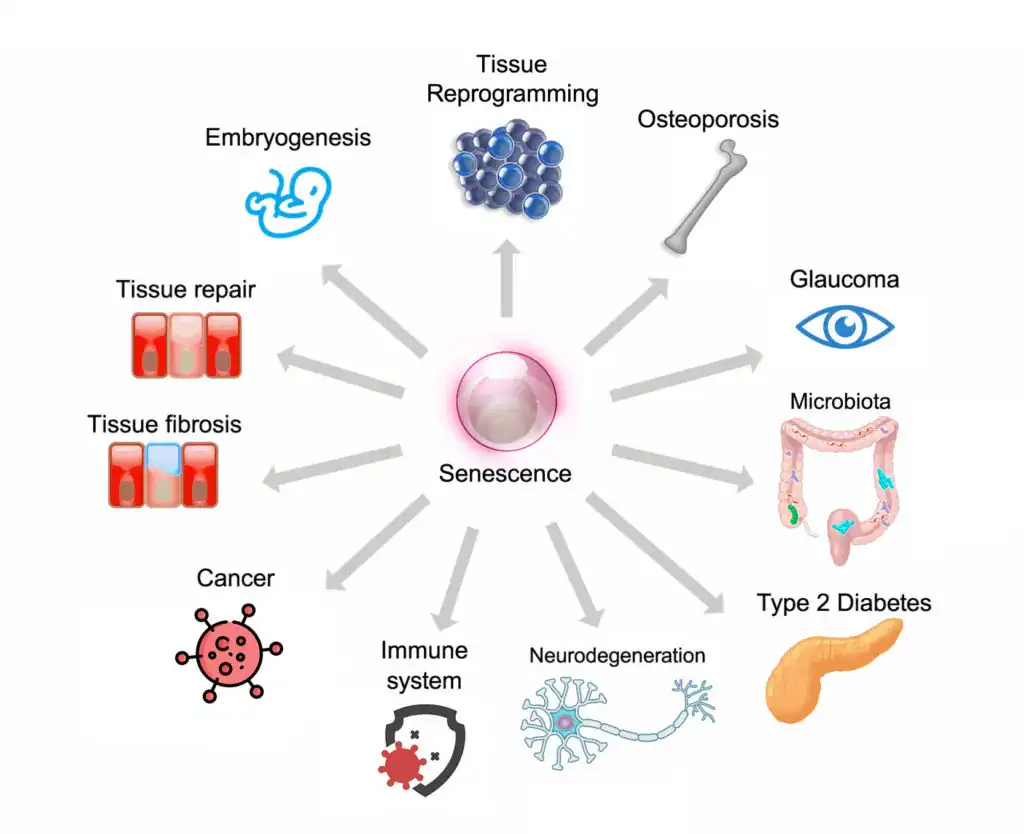
Cellular senescence, what some researchers call the “zombie cell” problem, is another mechanism that rarely appears in standard Long COVID treatment frameworks, although it may accidentally be addressed (albeit not thoroughly enough) through treatments with other prescribed purposes.
Senescent cells are cells that have stopped dividing but refuse to die. In the aftermath of a severe immune activation like COVID infection, the body can accumulate these cells in significant numbers. In fact, the spike protein seems to have be very skilled at producing senescent cells. These cells don’t do their normal jobs, but they also release a continuous stream of pro-inflammatory signaling molecules, the senescence-associated secretory phenotype (or SASP).
The result of senescent cell accumulation is a low-grade, chronic inflammatory state that can persist for years. Standard anti-inflammatory approaches don’t clear senescent cells. Senolytics, which are treatments that induce apoptosis in senescent cells, are rarely considered in clinical practice, let alone in Long COVID or Post-Vaccine Syndrome.
For patients where senescent cell burden is a significant contributor, which is all spike protein patients, treating everything else while ignoring this mechanism is like bailing water from a boat without fixing the leak.
3. They Apply Uniform Protocols to Non-Uniform Patients
We understand why this happens. Protocols are efficient. They can be standardized, taught, and scaled. If you’re running a practice that sees 50 Long COVID patients a week, a decision tree makes sense. Our practice model focuses on lower patient volumes for more personalized care and treatment. Why?
Long COVID patients are not uniform. The neurotransmitter profile of one patient – the specific pattern of catecholamine deficiency, glutamate dysregulation, and kynurenine pathway disruption – may look nothing like the next patient’s. The autoimmune burden, the degree of microclotting, the level of residual spike protein activity, the autonomic dysfunction pattern, may all vary enormously from patient to patient.
Our practice partner Scott Marsland, FNP-C, published a detailed case study that illustrates this complexity in just one patient, examining neurotransmitter changes across time and in response to specific interventions. The data showed 13 of 27 measured neurotransmitters were outside optimal range at baseline. The specific pattern of elevated glutamate suggesting excitotoxicity, paradoxically elevated serotonin alongside low tryptophan, and depleted catecholamines required a tailored response, not a standard protocol. And the picture changed meaningfully over seven months, requiring ongoing adjustment.
That is what individualized Long COVID care actually looks like.
4. They Over-Test and Under-Treat
There are particular kind of specialty practices that run $2,000–$5,000 in laboratory panels before doing much of anything. The testing is framed as “comprehensive” and “data-driven.” It feels thorough. As humans, we want to latch onto something concrete, like lab results. It gives us something to work at, and improve upon.
But here’s the honest clinical reality: in most Long COVID and PACVS patients, extensive testing rarely changes the initial treatment approach. The patterns we see across 3,500+ cases are recognizable. The likely mechanisms become apparent through careful history, symptom characterization, and clinical pattern recognition long before any lab results return.
Excessive testing delays treatment. It costs patients money they could have spent on interventions. And it creates an illusion of certainty in a condition that requires the intellectual honesty to acknowledge: we are treating this by thoughtful trial, observation, and adjustment. Running a panel and following a chart does not work for complex conditions like Long Covid and Post-Vaccine Syndrome. One day might turn up a normal lab result, and then many abnormalities the next testing period. Patients end up chasing ghosts.
And, by the way, if and when a $4,000 testing panel arrives that meaningfully guides pin-pointed treatment decisions tha deliver results, we will be the first ones to come back and edit this post.
5. They Treat the First Layer and Stop
Long COVID recovery, when it happens, typically unfolds across 9 to 18 months. Sometimes longer. The condition does not resolve in a single treatment arc, but requires ongoing attention to how the patient’s picture is shifting.
A treatment that was appropriate in month two may need modification by month five. An intervention that wasn’t relevant initially may become important as other issues resolve and different mechanisms become more apparent. The clinical work is iterative.
Many practices, particularly those operating at high volume or on a brief-consultation model, don’t have the infrastructure or clinical philosophy to support this. They prescribe an initial regimen and check in only when you schedule your next appointment. That interval is too long, and the flexibility to pivot is often not there.
What a Different Approach Looks Like
We want to be direct about what we actually do differently, not just what we criticize.
We start with clinical reasoning, not a panel. The first consultation at Leading Edge Clinic is 60 minutes. We are building a detailed picture of your symptom history, your illness trajectory, what you’ve tried, how you responded, and what the pattern suggests. That reasoning guides our initial approach, not a lab panel.
We think about mechanisms, not just symptoms. If you have fatigue, we want to understand whether it’s primarily metabolic, autonomic, inflammatory, or driven by a cellular danger response that hasn’t resolved. Different mechanisms call for different interventions.
We are honest about the trial-and-error nature of treatment. We don’t tell patients we’ve found the answer and here it is. We tell them: here is our best clinical hypothesis, here is the treatment we think is most likely to move things in the right direction, and here is how we’ll know if it’s working. We adjust based on what we observe.
We treat the evolving patient, not the initial presentation. Follow-up is built into how we work. As patients respond, we incorporate that information and adapt.
We consider mechanisms that others don’t. Cell danger response, cellular senescence, persistent spike protein activity, microclotting, neurological changes, autonomic dysfunction, immune dysregulation, MCAS, and other spike protein pathologies are all part of our clinical thinking. Not for every patient, but for the patients where these mechanisms are relevant, addressing them can be the difference between continued decline and meaningful recovery.
What You Should Ask Any Long COVID Specialist
If you’re evaluating whether a Long COVID practice is right for you, here are honest questions worth asking:
“What do you think is driving my specific symptoms?” A clinician who can give you a mechanistic hypothesis, specific to your history, and not a generic answer, is thinking carefully. A clinician who gives you the same answer they give everyone is running a protocol.
“What do you do when a treatment isn’t working?” The answer should involve active pivoting, consideration of alternative mechanisms, and willingness to try something different.
“How do you think about conditions like cell danger response or cellular senescence?” You’re not expecting a dissertation. But a blank look or a dismissive response tells you something about the depth of the clinical framework.
“How long do you expect treatment to take?” Honesty here matters. Anyone promising significant recovery in 6 to 8 weeks is either treating very mild cases or not being straight with you. The realistic timeline for meaningful improvement in complex Long COVID is 9 to 18 months.
A Note on What We Don’t Promise
We’ve seen enough patients and enough trajectories to say this plainly: approximately 80–85% of our patients achieve significant functional improvement over the course of treatment. That is a meaningful number, and we’re proud of it.
But 80–85% also means that 15–20% of patients don’t reach that threshold, at least not within our treatment window.
What we can promise is clinical honesty, genuine intellectual engagement with your case, and a willingness to keep thinking when the obvious approaches aren’t working.
If You’ve Already Tried Everything
If you’ve been through the conventional system, the university Long COVID clinics, the integrative medicine practices, the telehealth protocols – and you’re still significantly impaired – there may be value in a clinical framework that explicitly accounts for the mechanisms most others aren’t addressing.
We recognize that many of our patients come to us precisely because they’ve exhausted the obvious options and need something different.
A 60-minute initial evaluation gives us the opportunity to build a complete picture of your case: what you’ve tried, how you responded, what your symptom pattern suggests, and where we think there may be unexplored mechanistic territory. From that, we develop a realistic treatment roadmap, not a protocol applied to a category, but a clinical plan developed for your specific situation.
Long COVID and Post-Vaccine Syndrome not one disease. They don’t have one mechanism, they don’t respond to one protocol, and they don’t resolve on a predictable timeline.
The clinicians who are having the best outcomes with this condition are the ones who understand complexity, think in terms of mechanisms, are willing to adapt, and have the clinical experience to recognize patterns that don’t fit neatly into any category.
That is the medicine we practice. If you’ve been failed by other approaches and you’re still looking for meaningful progress, we’d be glad to talk.
Leading Edge Clinic specializes in Long COVID, Post-Vaccine Syndrome, and complex post-infectious illness. Our clinic has treated more than 3,500 patients with these conditions.
This article is for informational purposes and does not constitute medical advice. Individual results vary.
We have treated over 3,500 Long COVID and Post-Vaccine Syndrome cases since 2022. However, still, the treatments showing the most promise in clinical practice aren’t yet in the official guidelines.
This isn’t surprising. The gap between clinical innovation and institutional approval often takes years, sometimes decades, to close. That is, if they ever close at all. There is, of course, story after story of promising curative treatments purchased by pharmaceutical companies and immediately thrown in the filing cabinet of oblivion – innovation killed and stifled to maintain cash cow products that produce no meaningful results.
Now infamous, the time a Goldman Sachs analyst asked the quiet part out loud: “Is curing patients a sustainable business model?” The analyst when on to write in her report, “…such (curative) treatments offer a very different outlook with regard to recurring revenue versus chronic therapies. While this proposition carries tremendous value for patients and society, it could represent a challenge for genome medicine developers looking for sustained cash flow.”
Long COVID and Post-Vaccine Syndrome patients can’t wait to see if someone looks favorably at the economic viability of helping them with their severe and debilitating conditions. And if that endeavor is decidedly profitable (which it most certainly will be based on the current trajectory of severely ill spike protein patients), they can ill afford to wait the additional 5+ years for clinical research and testing for expensive, patented drugs that treat symptoms.
What follows is an evidence-based discussion of a small handful of treatments we’ve used successfully in clinical practice, why they work mechanistically, what the research shows, and why most physicians haven’t adopted them yet. This is by no means an exhaustive list. But, some treatments we thought were worth highlighting for one reason or another.
This represents real-world clinical experience combined with emerging research. The kind of information you need to have informed conversations with your healthcare provider.
Understanding the Treatment Gap
Before discussing specific treatments, it’s important to understand why there’s often a delay between what helps patients and what becomes “standard of care.”
Three Primary Barriers:
1. Regulatory Framework Most of these treatments are FDA-approved for other conditions but used “off-label” for Long COVID. While legal and common in medicine, off-label use requires physician comfort with clinical decision-making beyond established protocols. We saw during the pandemic that “off-label” suddenly became a dirty word, weaponized against certain drugs demonstrating promise in treatment. More on that later.
2. Evidence Timeline Rigorous clinical trials take 3-5 years from design to publication. Long COVID emerged in 2020. We’re only now seeing results from the first wave of controlled trials. Furthermore, these trials are often on patented therapies with high side effect profiles and little clinical efficacy.
3. Risk-Benefit Calculation Physicians must weigh potential benefit against professional liability, especially for treatments lacking specific FDA approval for Long COVID. Even when clinical rationale is strong. To us, the decision is easy. Integrity trumps all risk.
The result: Patients often wait years for treatments that clinical experience suggests could help now.
Treatment #1: Low-Dose Naltrexone (LDN)
What it is: Naltrexone at standard doses (50-100mg/day) treats opioid addiction. At lower doses (1-4.5mg/day), it functions as an immunomodulator with anti-inflammatory properties.
Clinical rationale for Long COVID:
Low-dose naltrexone works through multiple mechanisms relevant to Long COVID pathophysiology:
Immune modulation: Inhibits pro-inflammatory toll-like receptor 4 (TLR4), which drives cytokine production
Cytokine reduction: Decreases inflammatory markers including IL-6, TNF-alpha, and IL-1β
Ion channel restoration: A 2025 study demonstrated LDN restored TRPM3 ion channel function in Long COVID patients’ immune cells—significant because TRPM3 dysfunction impairs cellular energy production and immune response
Mast Cell Stabilization: By reducing immune reactivity and cytokine production, it also creates a more stabile environment, preventing histamine release from mast cells.
Neuroinflammatory Reduction: Reduces microglial activation in the brain, with 60% of users reporting reduction in anxiety, fatigue, and brain fog
Current evidence:
The NIH RECOVER program selected LDN for clinical trials, with enrollment beginning summer 2026. Existing data includes:
Meta-analysis of observational studies (n=155 across 4 studies): Moderate effect size for fatigue reduction (Hedges’ g = -0.74, p<0.001)
Quality of life improvements: SF-36 scores increased from 36.5 to 52.1 (p<0.0001) over 12 weeks
TRPM3 restoration study (Frontiers in Molecular Biosciences, 2025): Demonstrated objective improvement in immune cell calcium signaling
Safety profile: Excellent across multiple studies. Most common side effects are mild and transient (vivid dreams, slight headache in first 1-2 weeks)
Contraindications: Active opioid use, liver dysfunction
Clinical experience: In our practice, approximately 50-60% of Long COVID and Post-Vaccine Syndrome patients experience significant benefit from LDN. Response is most notable for fatigue, post-exertional malaise, and brain fog.
Typical response timeline: 8-12 weeks at therapeutic dose.
Prescribing approach:
Start low (0.5-1mg) to assess tolerance
Titrate slowly: increase by 0.5mg every 3-5 days
Target dose: 3-4.5mg daily
Taken at bedtime (may initially cause vivid dreams)
Requires compounding pharmacy
Why adoption is limited: Requires off-label prescribing, compounding pharmacy access, and physician comfort with immunomodulation. Many physicians prefer to wait for RECOVER trial results before prescribing. To us, it is shocking that it has taken this long to even get studies going on this low risk, high benefit option.
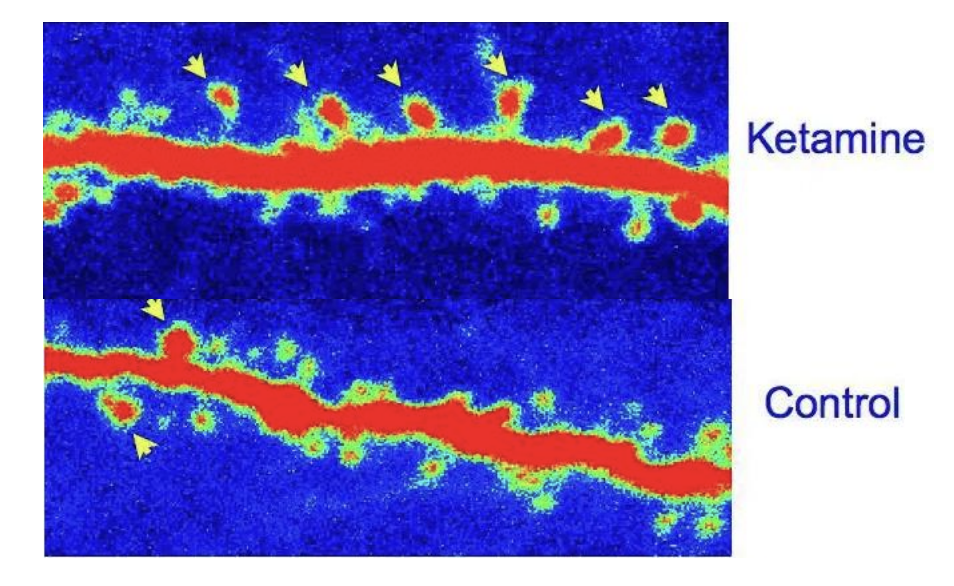
Treatment #2: Low-Dose Ketamine
What it is: Ketamine is an NMDA receptor antagonist originally used for anesthesia, now FDA-approved for treatment-resistant depression via the esketamine nasal spray (Spravato). We have written more extensively about its history, its mechanisms of action, and what we’ve seen in our Long Covid and Post-Vaccine Syndrome patients here
Clinical rationale for Long COVID and Post-Vaccine Syndrome:
Ketamine addresses multiple Long COVID and PACVS mechanisms:
Neuroinflammation reduction: Downregulates inflammatory cytokines (IL-6, IL-17A, TNF-alpha) that contribute to brain fog and cognitive dysfunction
Rapid-acting antidepressant: Unlike traditional SSRIs requiring 4-6 weeks, ketamine can show effects within hours to days, and takes a fundamentally different approach from serotonin based treatments
Chronic pain modulation: Effective for neuropathic pain through NMDA receptor antagonism
Current evidence:
Active clinical trials: University of British Columbia Phase 2 trial testing ketamine for Long COVID fatigue and cognitive symptoms (NCT identifier pending, 20 participants)
Case reports: Published cases demonstrating rapid improvement in treatment-resistant depression and suicidality in Long COVID patients. These reports are focused on psychological impacts. However, there are significant physiological benefits to treatment as well
Mechanism studies: Ketamine reduces specific inflammatory markers that correlate with Long COVID symptom severity
Combination therapy: German observational study showed promising results combining ketamine with repetitive transcranial magnetic stimulation (rTMS)
Administration routes:
Low-Dose Sublingual Ketamine: Although there are other administrative routes (IV, intranasal, etc…), to achieve therapeutic dosing for Long Covid and Post-Vaccine Syndrome patients, only low doses are needed. These doses can be achieved through sublingual administrations via compounded drops, or troches.
Clinical experience: Most dramatic improvements occur in patients with:
Severe fatigue with cognitive dysfunction
Chronic neuropathic pain
Persistent brain fog unresponsive to other interventions
Anxiety and depressive related disorders
Dysautonomia symptoms
Typical protocol: Daily sublingual drops or troches at minimally tolerable dose. Dosing dependent upon tolerability is based on glutamate imbalances, which are corrected over time with sublingual low-dose ketamine. Improvements are seen over a 6 month period.
Safety considerations:
Requires medical supervision and monitoring
Potential side effects with low-dose sublingual ketamine: Dissociation, minor euphoric feeling, anxiety during infusion
Contraindications: Active substance abuse (however, this can also be a treatment for substance abuse)
Not appropriate for all patients
Why adoption is limited: Off-label prescribing of low-dose sublingual ketamine for Long Covid and Post-Vaccine Syndrome is not something many clinicians are aware, let alone comfortable with. Its benefits are well-known in some psychiatric medicine circles for treatment resistant depression, but its effects on BDNF and neuronal healing are not yet mainstream for the treatment of other conditions, such as Long Covid, that impact brain health. It is a controlled substance, which means prescribers must have DEA licenses.
Treatment #3: Dimethyl Sulfoxide (DMSO)
What it is:Dimethyl sulfoxide(DMSO) is a chemical solvent and prescription medication primarily used to treat painful bladder syndrome (interstitial cystitis). It is known for its ability to rapidly penetrate skin and membranes, acting as an anti-inflammatory and analgesic agent.
Clinical rationale for Long COVID and Post-Vaccine Syndrome:
Some argue that DMSO is the most suppressed therapeutic in modern medicine because it works too well for too many things. You’ll remember from earlier in this article what the Goldman Sachs analyst said about effective, curative treatments. When the FDA banned DMSO in 1965 (despite overwhelming safety data), thousands of patients with debilitating conditions lost access to a therapy that was giving them their lives back. The parallels to how Long COVID and Post-Vaccine Syndrome patients are being dismissed today are not coincidental.
Here’s what makes DMSO uniquely suited for spike protein disease:
The Spike-Protein Connection: Why DMSO Makes Mechanistic Sense
If persistent spike protein is driving Long COVID and Post-Vaccine Syndrome pathology—and mounting evidence suggests it is—then DMSO addresses nearly every downstream mechanism we see clinically:
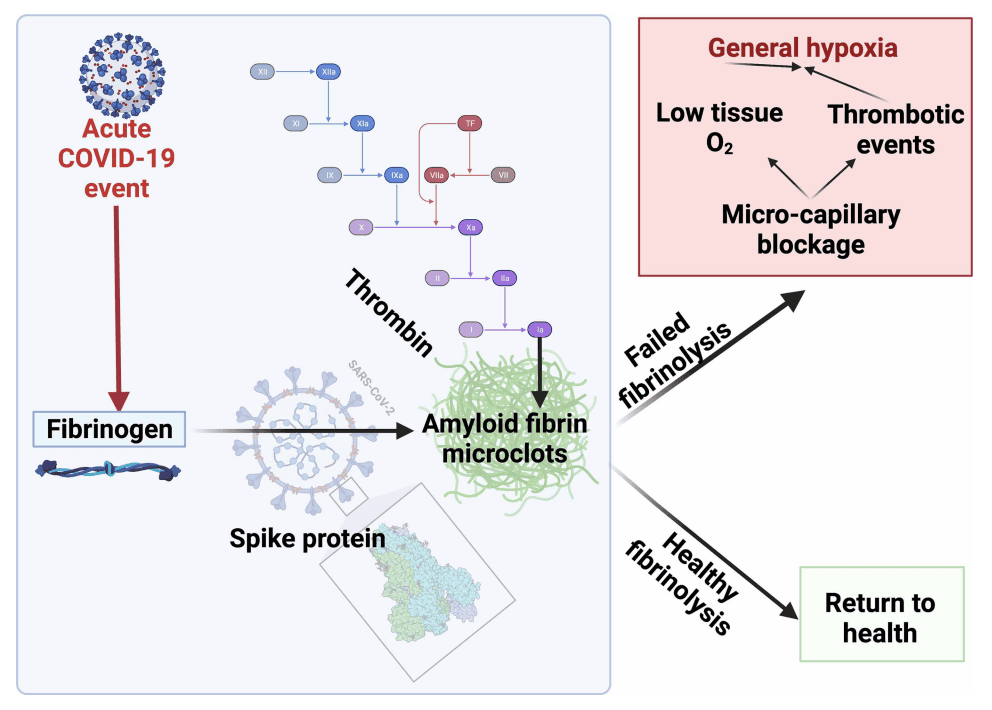
1. Protein Misfolding and Amyloid Fibrin Microclotting
DMSO is a chemical chaperone. It stabilizes protein folding and, critically, dissolves amyloid aggregates.
At least 40 studies have demonstrated DMSO’s ability to solubilize amyloid fibrils and enable the body to break them down. If spike protein is creating misfolded proteins or amyloid-like microclots (the leading hypothesis for many Long COVID and PACVS symptoms), DMSO has a direct mechanism of action:
Prevents proteins from aggregating into pathologic forms
Dissolves existing amyloid deposits
Allows the body to clear these aggregates through normal elimination pathways
This isn’t theoretical, or even in vitro evidence. DMSO has successfully treated amyloidosis in humans—a condition characterized by insoluble protein aggregation causing organ damage. Same mechanism, different protein.
The microclotting angle: DMSO is also a powerful platelet deaggregator and anticoagulant:
Inhibits platelet aggregation induced by ADP, collagen, arachidonic acid, and platelet-activating factor
Blocks tissue factor (TF) expression—the key link between inflammation and clotting
Unlike aspirin or heparin, it does this without bleeding risk
If microclots are clogging your microcirculation and causing tissue hypoxia, DMSO addresses it directly while simultaneously improving blood flow to oxygen-starved tissues.
2. Autoimmunity
Spike-triggered autoimmunity is one of the most devastating Long COVID mechanisms. DMSO has decades of evidence treating autoimmune conditions that conventional medicine still can’t touch:
Lupus – reduces symptoms, often allowing steroid reduction
Multiple sclerosis – stops progression in many cases, improves symptoms
Rheumatoid arthritis – 70-80% response rate in multiple studies
Scleroderma – one of the few things that works for this “untreatable” condition
Interstitial cystitis – the only FDA-approved use for DMSO (because the evidence was impossible to suppress)
Sjögren’s syndrome – dramatically improves dry mouth/eyes in published case series
Improves microcirculation – documented in studies using radioactive isotope imaging
Treats vasospasm – successfully used for Raynaud’s syndrome, peripheral neuropathy, complex regional pain syndrome
Clinical studies show DMSO:
Eliminates symptoms in 50% of Raynaud’s patients
Treats diabetic peripheral neuropathy and prevents amputations
Resolves varicose veins (sometimes within minutes of IV administration)
Improves circulation in thrombophlebitis and peripheral artery disease
If spike-ACE2 interaction is damaging your vasculature, DMSO protects and heals blood vessels.
4. Neurological Protection and Small Fiber Neuropathy
Small fiber neuropathy is the #4 most common vaccine injury symptom. It’s also prevalent in Long COVID.
DMSO selectively blocks C-fibers and A-delta fibers—the exact nerve fibers responsible for burning pain, electrical shocks, pins-and-needles, and the agonizing dysesthesias of small fiber neuropathy.
Mechanism:
Blocks nerve conduction in small pain fibers without affecting larger motor/sensory fibers
Suppresses NMDA and AMPA receptor activity (central pain sensitization)
Blocks excessive calcium/sodium influx into pain-transmitting neurons
Does NOT create tolerance (unlike opioids—often becomes MORE effective over time)
Additionally, DMSO crosses the blood-brain barrier and:
Protects neurons from death following ischemia/hypoxia
Reduces neuroinflammation
Treats brain fog, cognitive dysfunction (reported extensively in Long COVID patients using DMSO)
Has successfully treated traumatic brain injuries, strokes, spinal cord injuries in studies the FDA ignored
5. Organ Protection and Healing
DMSO doesn’t just reduce symptoms, it heals damaged tissue. This is critical for Long COVID and Post-Vaccine Syndrome patients with organ involvement (which would be most patients):
Lungs:
Reduces pulmonary fibrosis (case reports of transplant candidates recovering)
Treats COPD, asthma exacerbations
Improves oxygenation in respiratory insufficiency
81% of patients with chronic respiratory failure improved without hospitalization in one study
Dosing: We start with topical and/or oral dosing based on specific patient needs, titrating appropriately based on response and tolerability. Some patients seek out IV administration for more aggressive treatment, though this is logistically challenging outside specialized clinics.
Expected timeline:
Acute symptoms (pain, inflammation): Often improve within hours to days
Chronic conditions: 4-7 days to start seeing benefit, 6-8 weeks for sustained improvement
DMSO often becomes MORE effective with continued use (opposite of pharmaceutical tolerance)
Contraindications and cautions:
Pregnancy/breastfeeding – inadequate safety data (though one study showed safe use for infertility)
Active skin infections – DMSO can carry surface toxins into the body; ensure skin is clean before application
Severe liver or kidney dysfunction – use with caution, monitor closely
Concurrent DMSO + PRP injections – may reduce PRP efficacy due to platelet inhibition
Allergic reactions – rare (~1 in 2000) but possible; start with low concentration to assess tolerance
Skin irritation with topical use (concentration-dependent, often resolves with continued use)
Nausea (uncommon with appropriate dosing)
Why You Haven’t Heard About This
The FDA banned DMSO research in 1965 based on a fabricated safety concern (lens opacities in dogs—which never occurred in any other species or in humans). Despite Congressional hearings, outcry from patients and physicians, and a former Secretary of Health and Human Services championing it after using DMSO to treat his wife’s terminal cancer pain, the FDA never relented.
Why? DMSO threatened too many profitable drug markets.
In 1966, over 1,000 researchers presented evidence at the Waldorf Astoria. Zero withdrew their papers despite FDA pressure. The data was overwhelming.
Sixty years later, patients are still suffering from conditions DMSO could treat—because the FDA decided your access to effective medicine was less important than protecting pharmaceutical profits.
For Long COVID patients failed by the medical establishment, DMSO represents what medicine should have been: safe, effective, accessible, and focused on healing rather than management.
Bottom line on DMSO for Long COVID:
If persistent spike protein is causing:
Protein misfolding → DMSO refolds and stabilizes proteins
Amyloid microclots → DMSO dissolves aggregates and prevents platelet aggregation
Organ damage → DMSO protects lungs, gut, heart, kidneys
The mechanism isn’t speculative. The evidence isn’t anecdotal. This is decades of suppressed research finally reaching patients who need it.
Treatment #4: Microcurrent Therapy
What it is: Microcurrent therapy delivers sub-sensory electrical currents in the microampere range — currents so small they mimic the body’s own bioelectrical signals. We commonly have recommended the Arc Microtech device. The Arc device was engineered by Ian Thirkell, a retired English detective who spent years studying the bioelectricity research of Dr. Robert O. Becker after his wife handed him three of Becker’s books and told him to go learn something useful.
The scientific foundation is worth understanding. Becker was an orthopedic surgeon and researcher at the VA Hospital in Syracuse, New York, who spent decades studying how the body uses electrical signals to heal. He discovered that injury generates a measurable shift in voltage at the wound site — a “current of injury” — that initiates the healing process. He demonstrated that applying tiny electrical currents could stimulate partial limb regeneration in rats (published in Nature, 1972) and developed techniques using electrically generated silver ions to fight antibiotic-resistant infections and promote tissue regeneration in human patients. His core insight, detailed in his landmark book The Body Electric (1985): the body operates on a bioelectrical control system that can be supported and restored through the careful application of currents matching the body’s own frequencies. The ARC device is built directly on this principle.
Clinical rationale for Long COVID and Post-Vaccine Syndrome:
ATP production enhancement: The landmark 1982 study by Cheng et al. demonstrated that microcurrent stimulation in the 100-500 microampere range increased ATP production by up to 500% in treated tissue, while increasing amino acid transport by 30-40% and enhancing protein synthesis. When current was increased into the milliampere range used by TENS units, ATP production actually decreased. This distinction matters enormously: Long COVID and Post-Vaccine Syndrome patients have documented mitochondrial dysfunction. A 2025 study in Annals of Medicine confirmed that immune cells from Long COVID patients exhibit aberrant ATP synthase function, resulting in diminished cellular energy availability. The spike protein — whether from viral reservoirs or circulating post-vaccination — impairs oxidative phosphorylation, the process responsible for 90% of cellular energy production. Fatigue, post-exertional malaise, brain fog, exercise intolerance — these are manifestations of cells that cannot produce adequate energy (although there is greater detail as to what is happening here, some of this is detailed in our prior article on cell danger response). Microcurrent directly targets this deficit.
Inflammation reduction: Microcurrent reduces inflammatory markers and promotes resolution of swelling through enhanced circulation and lymphatic drainage — relevant to the chronic systemic inflammation driving Long COVID and Post-Vaccine Syndrome symptoms
Tissue repair and cellular regeneration: Building on Becker’s work, microcurrent stimulates fibroblast activity, enhances collagen synthesis, and promotes angiogenesis. For patients with endothelial damage and microclotting from spike protein, these repair mechanisms are critical. We have seen patients in heart failure restore their ejection fraction back to well over the CHF baseline.
Autonomic and neurological support: Clinical observations from our practice and colleagues in the UK suggest meaningful benefit for patients with autonomic dysfunction, anxiety, depression, and PTSD — conditions that frequently accompany Long COVID and Post-Vaccine Syndrome
One framing we find useful: supplements that support mitochondrial function — CoQ10, B vitamins, magnesium — are static interventions for what is fundamentally a dynamic process. They provide raw materials. Microcurrent is a dynamic intervention: it actively stimulates the cellular machinery to do its job. The two approaches are complementary, not competing.
Current evidence:
Cheng et al. (1982): Foundational study demonstrating 500% ATP increase at therapeutic microcurrent levels, with concurrent increases in amino acid transport and protein synthesis Becker’s published work (1961-1998): Decades of peer-reviewed research on bioelectrical control of regeneration, published in Nature, Science, and other major journals Modern reviews: A 2025 narrative review confirmed microcurrent’s role in enhancing ATP synthesis, improving mitochondrial efficiency, and activating tissue repair mechanisms No randomized controlled trials specific to microcurrent for Long COVID exist, and they may never — putting it in the same category as most treatments on this list when they were first adopted clinically.
Clinical experience: In our practice, over 500 patients have used the ARC device. It has been a reliable and safe recommended interventions for a few years now.
Most consistent improvements:
Fatigue — the most reliably reported benefit, typically noticeable after approximately six weeks of consistent use Pain and inflammation — reduced swelling and bruising, notably effective for patients on anticoagulation therapy Cardiac function — we have observed cases of improved cardiac ejection fraction with sustained use, corroborated by colleagues in the UK Brain fog and cognitive function — improvements likely related to enhanced cellular energy production and reduced neuroinflammation Anxiety and trauma-related symptoms — consistent with observations from military psychiatrists using microcurrent for treatment-resistant PTSD
Benefit is cumulative. More consistent use produces greater results.
Typical protocol:
Program 1 (100% anti-inflammatory): At least one 3-hour cycle daily for two months Program 2 (50% anti-inflammatory, 50% cellular repair): At least one 3-hour cycle daily for two weeks Program 3 (25% anti-inflammatory, 75% cellular repair): At least one 3-hour cycle daily for two weeks Then rotate: One week each of Programs 1, 2, and 3, repeating continuously
Worn on the arm or leg (most patients prefer above the ankle). The strap should be fitted but not tight — two fingers should fit between strap and skin. Tightness inhibits circulation and reduces benefit.
Response timeline: Most patients notice benefit after approximately six weeks. Some report improvement within days, particularly for pain and inflammation. However, some patients even report improved energy in just days.
Safety considerations:
Excellent safety profile — these are sub-sensory currents operating at the same magnitude as the body’s own cellular electrical signaling Approximately 5% of patients experience initial sensitivity (nausea, dizziness), managed by starting with very short sessions and gradually increasing No significant adverse effects observed in our patient population Safe for use alongside other treatments, including anticoagulation Contraindications: Active implanted electrical devices (pacemakers, defibrillators)
Why adoption is limited: Microcurrent therapy sits entirely outside the pharmaceutical paradigm. There is no drug to prescribe, no procedure to bill for, and no pharmaceutical company funding trials. Becker himself faced significant institutional resistance throughout his career — his research challenged the chemical-mechanistic model of biology, and his opposition to electromagnetic pollution put him at odds with powerful interests. The ARC Microtech is a small, family-owned UK company without resources for large-scale clinical trials. And the concept that a wearable device delivering imperceptible electrical currents can meaningfully impact chronic illness strikes most conventionally trained physicians as implausible, despite decades of published research supporting the underlying science.
Our perspective: Microcurrent therapy, and specifically the ARC device, is one of the most underappreciated tools in our clinical arsenal. It is non-invasive, has an excellent safety profile, produces cumulative benefit, and directly addresses what may be the single most important pathological mechanism in Long COVID and Post-Vaccine Syndrome: mitochondrial energy failure. For a condition where the body has lost its ability to produce adequate energy, providing it with the bioelectrical signal to restore that production isn’t alternative quackery — it’s the application of proven biophysics.
Conflicts of Interest: We do offer a discount code for the ARC Microtech device. Using code USARCLEC at checkout on the ARC website provides a $20 discount to ordering customers. ARC also provides us with $20. However, we have never stashed this money away in a bank account. We have historically used this money to re-invest into devices for patients who can not afford to invest in this special device.
Treatment #5: Ivermectin
The controversial treatment that requires honest discussion.
Ivermectin became one of the most politicized medications in modern history. That makes it difficult to have rational, evidence-based conversations about its potential role in Long COVID and Post-Vaccine Syndrome.
Here’s what we actually know:
What it is: An antiparasitic medication on the WHO’s List of Essential Medicines, with an excellent 40-year safety record from billions of doses administered globally.
Theoretical mechanisms for Long COVID and Post-Vaccine Syndrome:
1. Spike Protein and ACE2 Receptor Interaction: This is perhaps the most relevant mechanism for Long COVID and Post-Vaccine Syndrome. Multiple molecular docking studies have demonstrated that ivermectin binds to:
The spike protein receptor-binding domain (RBD): Where the spike protein attaches to ACE2 receptors
The spike-ACE2 complex interface: Specifically between leucine 91 of the spike protein and histidine 378 of the ACE2 receptor
The N-terminal domain (NTD): Which controls initial viral attachment to cell membranes
Binding energy studies show strong affinity (-18 kcal/mol), suggesting ivermectin may physically interfere with spike protein attachment to ACE2 receptors.
Why this matters for Long COVID and Post-Vaccine Syndrome: If persistent spike protein (either from viral reservoirs or circulating spike) is driving symptoms—a leading hypothesis in Long COVID and Post-Vaccine Syndrome pathophysiology—ivermectin’s ability to bind both spike protein and ACE2 receptors could theoretically:
Reduce spike-mediated inflammation and endothelial damage
2. Additional antiviral mechanisms:
TMPRSS2 binding: Ivermectin binds to TMPRSS2, a protease that activates spike protein for cell entry
Viral replication inhibition: Demonstrated in vitro inhibition of SARS-CoV-2 replication
Multiple viral protein targets: Binds to main protease (Mpro), RNA-dependent RNA polymerase (RdRp), and nucleocapsid proteins
3. Anti-inflammatory effects:
Inhibits nuclear import of inflammatory transcription factors
Reduces cytokine production (IL-6, TNF-alpha, IL-1β)
Modulates immune response through multiple pathways
Important concentration caveat: While docking studies predict strong binding, debate exists about whether therapeutically achievable concentrations in humans are sufficient for these effects. One 2024 study suggested effective spike binding required concentrations 100-1000x the approved dosage in their assay system, though other studies and clinical observations suggest benefit at standard doses. Our clinical observations suggest extremely safe dosing ranges are effective in about 70% of patients.
The discrepancy may relate to:
Differences between in vitro assays and in vivo conditions
Tissue concentration versus serum concentration
Individual pharmacokinetic variation
Duration of exposure in chronic dosing versus single-dose studies
The evidence landscape:
The data on ivermectin for acute COVID-19 was mixed, politicized, and contentious. For Long COVID specifically:
No published randomized controlled trials
Mechanistic rationale exists
Clinical experience varies among practitioners. Our experience suggests a 70% positive clinical response rate
Clinical experience: In our practice, we’ve observed a subset of patients—approximately 70%—who report improvement when ivermectin is included as part of a comprehensive treatment protocol.
Important caveats:
Not a monotherapy; used as part of multi-modal approach
Standard anti-parasitic dosing (not megadoses)
Drug interactions exist
Why adoption is limited: The political controversy surrounding ivermectin creates significant professional risk for physicians who prescribe it, even for legitimate clinical indications. Many state medical boards have issued warnings, and physicians face potential peer censure. Dr. Kory had his board certifications revoked for promoting its use in acutely ill COVID patients, even in spite of positive clinical responses.
Our perspective: With Dr. Kory having testified before the Senate about COVID treatments and faced professional consequences for advocating treatments outside the mainstream, we believe in the efficacy of ivermectin based on excellent safety profile, low cost, and high clinical response rates.
The question for any treatment should be: What does the evidence show, what is the safety profile, and what is the clinical experience?
For ivermectin in Long COVID and Post-Vaccine Syndrome: Mainsteam evidence is limited, the safety profile is excellent, and our clinical experience is positive.
Whether to try it should be an informed decision between patient and physician, weighing potential benefits against minimal risks.
Treatment #6: Anticoagulation Therapy
What it is: Blood-thinning medications ranging from aspirin to low-dose anticoagulants.
Clinical rationale:
Growing evidence suggests microclots may play a role in Long COVID:
Microclot hypothesis: Persistent microclotting causing tissue hypoxia and symptoms
Proven benefit in acute COVID: Anticoagulation improves outcomes in hospitalized patients
Current evidence: Mechanistically compelling. Clinical trials underway but results pending.
Clinical experience: Some patients show improvement with aspirin or low-dose anticoagulation. Requires careful patient selection and monitoring.
Safety considerations: Bleeding risk requires careful assessment. Not appropriate for all patients.
Why adoption is limited: Balancing benefit versus bleeding risk requires individualized assessment. Physicians appropriately cautious about anticoagulating without clear indication.
The Gap Between Evidence and Practice
Every treatment discussed here shares common characteristics:
Mechanistic rationale based on Long COVID and PACVS pathophysiology
Existing clinical experience supporting use
Acceptable safety profiles when used appropriately
Real clinical results within our treatment of over 3,500 Long Covid and Post-Vaccine Syndrome patients
Yet most physicians haven’t adopted them. Why?
The Institutional Reality:
Evidence requirements: Institutions typically require randomized controlled trials before treatment adoption. These trials take years.
Liability concerns: Off-label prescribing, while legal, increases perceived malpractice risk.
Guideline absence: Without official clinical guidelines, physicians lack institutional backing for treatment decisions.
Professional pressure: Medical boards, peer review, and institutional policies create incentives to wait for official recommendations.
This creates a gap: Patients suffering now while waiting for evidence that may take years to generate.
What You Should Know
These Treatments Aren’t Magic Bullets
Long COVID and Post-Vaccine Syndrome are heterogeneous and complex. Treatment response varies significantly between patients.
The ideal scenario would be completed randomized controlled trials for each treatment.
What we actually have:
Mechanistic understanding (how they should work)
Clinical experience (what we’ve observed)
Emerging trial data (what’s being formally tested)
Urgent patient need (can’t wait years for perfect evidence)
The challenge: Balancing the desire for perfect evidence with the reality of patients suffering now.
This Requires Specialized Care
Optimal Long COVID and Post-Vaccine Syndrome treatment requires a clinician who:
Understands complex post-viral illness
Can navigate off-label prescribing appropriately
Will monitor carefully for adverse effects
Knows when to adjust or discontinue treatment
Can integrate multiple therapeutic modalities
Not all physicians have this expertise or comfort level.
Clinical Outcomes
In our practice of 3,500+ Long COVID patients:
80-85% achieve significant functional improvement
This means:
Return to work (often with modifications initially)
Ability to exercise (frequently at reduced level initially)
Brain fog resolved or significantly improved
Fatigue reduced to manageable levels
Quality of life substantially better
Realistic timeline: 9-18 months on average
Long COVID and Post-Vaccine Sydnrome are chronic conditions requiring sustained treatment. Promises of rapid recovery are unrealistic for most patients.
Finding Appropriate Care
If you’re considering these treatments:
1. Informed discussion with your current physician Share this information. Ask if they’re willing to consider these approaches.
2. Seek Long COVID expertise Find physicians with specific experience treating post-viral illness.
3. Consider telemedicine options Some Long COVID and PACVS specialists work across state lines via telemedicine.
4. Join support communities Other patients can recommend physicians with Long COVID expertise.
5. Be your own advocate Come prepared with questions. Understand the rationale. Participate actively in treatment decisions.
The Bottom Line
Long COVID and PACVS treatment requires:
Integration of emerging research
Clinical judgment based on experience
Willingness to use approved medications for new indications
Patient-centered approach to risk-benefit analysis
Honest acknowledgment of uncertainty
Not all physicians are equipped or willing to practice this way. The traditional model of “wait for definitive evidence” serves patients poorly when that evidence is years away.
At our practice, we integrate the best available evidence with clinical experience from over 3,500 cases. We’re transparent about what we know, what we don’t know, and what we’ve observed.
This represents clinical medicine as it should be practiced: Thoughtful, evidence-informed, patient-centered, and unafraid of reasonable uncertainty.
If you’re a Long COVID or Post-Vaccine Syndrome patient seeking care that integrates clinical experience with emerging research, we treat complex post-viral cases at Leading Edge Clinic. Our approach is based on 3,500+ patient encounters, current medical literature, and individualized treatment planning.
Baldwin K, Wanson A, Gilecki L-A, Dalton C, Peters E, Halpape K. Intranasal ketamine as a treatment for psychiatric complications of long COVID: a case report. Mental Health Clinician. 2023;13(5):239-243. doi:10.9740/mhc.2023.10.239. PMC10732124. https://pmc.ncbi.nlm.nih.gov/articles/PMC10732124/
Evaluating the Neuromodulatory Effect of Ketamine in Long COVID-19. ClinicalTrials.gov Identifier: NCT06821087. University of British Columbia. https://clinicaltrials.gov/study/NCT06821087
Rolle C, Scheib M, Frank A, Russ I. Treatment of Chronic Fatigue Syndrome (CFS) in Post-SARS-CoV-2 Infection through combined outpatient Neuromodulation Therapy with Repetitive Transcranial Magnetic Stimulation (rTMS) and Ketamine IV Therapy — A Case Series. International Clinical Medical Case Reports Journal. https://ketaminplus.com/en/medical-studies
Zanos P, Moaddel R, Morris PJ, et al. Ketamine and ketamine metabolite pharmacology: insights into therapeutic mechanisms. Pharmacological Reviews. 2018;70(3):621-660. doi:10.1124/pr.117.015198.
Treatment #3: DMSO
Amyloid fibril dissolution / chemical chaperone:
Dzwolak W, Loksztejn A, Smirnovas V. Noncooperative dimethyl sulfoxide-induced dissection of insulin fibrils: toward soluble building blocks of amyloid. Biochemistry. 2009;48(26):6272-6284. https://pubmed.ncbi.nlm.nih.gov/19385641/
Kardos J, Yamamoto K, Hasegawa K, et al. Dissolution of beta2-microglobulin amyloid fibrils by dimethylsulfoxide. Journal of Biological Chemistry. 2003;278(24):21222-21227. https://pubmed.ncbi.nlm.nih.gov/12944383/
Hoshino M, Katou H, Hagihara Y, et al. Dimethylsulfoxide-quenched hydrogen/deuterium exchange method to study amyloid fibril structure. Biochimica et Biophysica Acta (BBA) – Biomembranes. 2007;1768(8):1886-1899. https://www.sciencedirect.com/science/article/pii/S0005273607000703
Iwai A, Yoshida T, Saito T, et al. Studies on biological actions of dimethyl sulfoxide in familial amyloidosis. Annals of the New York Academy of Sciences. 1983;411:52-64. https://pubmed.ncbi.nlm.nih.gov/6576722/
Amemori S, Iwakiri R, Ootani H, et al. Oral dimethyl sulfoxide for systemic amyloid A amyloidosis complication in chronic inflammatory disease: a retrospective patient chart review. Journal of Gastroenterology. 2006;41:444-449. https://link.springer.com/article/10.1007/s00535-006-1792-3
Asmis LM, Bazargan A, Pellegrin M, et al. DMSO inhibits human platelet activation through cyclooxygenase-1 inhibition. A novel agent for drug eluting stents? Biochemical and Biophysical Research Communications. 2010;391(4):1629-1633. https://pubmed.ncbi.nlm.nih.gov/20035720/
Saeed SA, Rasheed H, Ali TH, et al. Effects of dimethyl sulphoxide on aggregation of human blood platelets. Experimental and Molecular Pathology. 1987;46(2):159-169. https://pubmed.ncbi.nlm.nih.gov/2880990/
Rosenblum WI. Dimethyl sulfoxide effects on platelet aggregation and vascular reactivity in pial microcirculation. Annals of the New York Academy of Sciences. 1983;411:110-119. https://pubmed.ncbi.nlm.nih.gov/6410963/
Rosenblum WI. Dimethyl sulfoxide (DMSO) and glycerol, hydroxyl radical scavengers, impair platelet aggregation within and eliminate the accompanying vasodilation of, injured mouse pial arterioles. Stroke. 1982;13(1):35-39. https://www.ahajournals.org/doi/10.1161/01.str.13.1.35
Cheng N, Van Hoof H, Bockx E, et al. The effects of electric currents on ATP generation, protein synthesis, and membrane transport in rat skin. Clinical Orthopaedics and Related Research. 1982;(171):264-272.
Becker RO. Stimulation of partial limb regeneration in rats. Nature. 1972;235(5333):109-111.
Becker RO, Spadaro JA. Electrical stimulation of partial limb regeneration in mammals. Bulletin of the New York Academy of Medicine. 1972;48(4):627-641.
Becker RO, Chapin S, Sherry R. Regeneration of the ventricular myocardium in amphibians. Nature. 1974;248(444):145-147.
Becker RO, Selden G. The Body Electric: Electromagnetism and the Foundation of Life. William Morrow & Company; 1985.
Becker RO. Iontopheretic system for stimulation of tissue healing and regeneration. US Patent 5814094A. 1998.
Jonik S, Rothka AJ, Cherin N. Investigating the therapeutic efficacy of microcurrent therapy: a narrative review. Journal of Rehabilitation Medicine. 2025. PMC12357078. https://pmc.ncbi.nlm.nih.gov/articles/PMC12357078/
Piras A, Trofè A, Piperi I, et al. Physiological effects of microcurrent and its application for maximising acute responses and chronic adaptations to exercise. European Journal of Applied Physiology. 2022. https://link.springer.com/article/10.1007/s00421-022-05097-w
Lehrer S, Rheinstein PH. Ivermectin docks to the SARS-CoV-2 spike receptor-binding domain attached to ACE2. In Vivo. 2020;34(5):3023-3026. PMC7652439. https://pmc.ncbi.nlm.nih.gov/articles/PMC7652439/
Eweas AF, Alhossary AA, Abdel-Moneim AS. Molecular docking reveals ivermectin and remdesivir as potential repurposed drugs against SARS-CoV-2. Frontiers in Microbiology. 2021;11:592908. doi:10.3389/fmicb.2020.592908.
Ahmad S, Waheed Y, Abro A, Abbasi SW, Ismail S. Molecular screening of glycyrrhizin-based inhibitors against ACE2 host receptor of SARS-CoV-2. Structural Chemistry. 2021;32:1441-1452.
[2024 NTD binding study — Ivermectin binds spike N-terminal domain across variants including KP.3. Viruses (MDPI). 2024.]
Treatment #6: Anticoagulation Therapy
Kell DB, Laubscher GJ, Pretorius E. A central role for amyloid fibrin microclots in long COVID/PASC: origins and therapeutic implications. Biochemical Journal. 2022;479(4):537-559. doi:10.1042/BCJ20220016. https://portlandpress.com/biochemj/article/479/4/537/230829/
Pretorius E, Venter C, Laubscher GJ, et al. Prevalence of symptoms, comorbidities, fibrin amyloid microclots and platelet pathology in individuals with Long COVID/Post-Acute Sequelae of COVID-19 (PASC). Cardiovascular Diabetology. 2022;21(1):148. doi:10.1186/s12933-022-01579-5. https://link.springer.com/article/10.1186/s12933-022-01579-5
Pretorius E, Vlok M, Venter C, et al. Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovascular Diabetology. 2021;20:172. doi:10.1186/s12933-021-01359-7.
Grobbelaar LM, Venter C, Vlok M, et al. SARS-CoV-2 spike protein S1 induces fibrin(ogen) resistant to fibrinolysis: implications for microclot formation in COVID-19. Bioscience Reports. 2021;41(8):BSR20210611. doi:10.1042/BSR20210611.
Kruger A, Vlok M, Turner S, et al. Proteomics of fibrin amyloid microclots in long COVID/post-acute sequelae of COVID-19 (PASC) shows many entrapped pro-inflammatory molecules that may also contribute to a failed fibrinolytic system. Cardiovascular Diabetology. 2022;21(1):190. doi:10.1186/s12933-022-01623-4. PMC9491257. https://pmc.ncbi.nlm.nih.gov/articles/PMC9491257/
Libby P, Lüscher T. COVID-19 is, in the end, an endothelial disease. European Heart Journal. 2020;41(32):3038-3044. doi:10.1093/eurheartj/ehaa623.
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. All treatments discussed require physician supervision. Consult a qualified healthcare provider before starting any new treatment. Individual results vary. Treatment decisions should be made in consultation with your physician based on your specific medical history and circumstances.
If you developed POTS (Postural Orthostatic Tachycardia Syndrome) after COVID infection or vaccination, you’ve probably been told to:
Drink more water and increase salt
Wear compression stockings
Try beta-blockers or midodrine
Do gradual exercise reconditioning
And maybe you’ve tried all of these. Some helped a little. But you’re still dealing with:
Racing heart when you stand up
Dizziness and lightheadedness
Extreme fatigue after being upright
Brain fog that worsens throughout the day
Feeling like you’re going to pass out
Significant symptom burden first thing in the morning
Here’s what we’ve learned after treating thousands of Long COVID and Post-Vaccine Syndrome patients with POTS:
Standard POTS treatments address the symptoms. But in 70% or more of the patients who come to us, there’s an underlying structural problem that’s driving the whole thing. A problem that most doctors don’t know to check for.
And when we fix this underlying problem? Many patients see dramatic improvement, sometimes within days of treatment.
The Hidden Problem Most Doctors Miss
After treating patients with post-viral and post-vaccine POTS since 2020, we’ve found something striking:
Over 70% of our POTS patients have significant venous compression in their pelvis.
Specifically, compression of the left common iliac vein, which is the major vein that drains blood from your left leg back to your heart.
This isn’t some fringe condition. Research shows:
69% of POTS patients have significant iliac vein compression (compared to 40% of healthy controls)
Up to 80% of POTS patients have some form of pelvic venous insufficiency
Yet most doctors never evaluate for it
Why does this matter?
Because if your POTS is being driven by poor venous return to your heart, all the salt and compression stockings in the world won’t fix the underlying problem.
It’s like trying to fill a bucket that has a hole in the bottom. You can keep pouring water (blood volume expansion, medications), but if the drainage system is blocked, you’re not solving the actual issue.
What Is Iliac Venous Compression?
Your left common iliac vein sits behind your right common iliac artery. In the normal anatomy, this is fine. Blood flows through both vessels without issue.
But in many people, especially after spike protein exposure from COVID or vaccination, the vein gets compressed by the artery sitting on top of it.
This compression is called May-Thurner Syndrome or iliac venous compression syndrome.
What happens when this vein is compressed?
Blood from your left leg can’t return to your heart efficiently
Blood pools in your lower body, worsened by postural changes such as standing
Less blood returns to your heart
Your heart has to beat faster to maintain blood pressure (hello, POTS)
You get all the classic POTS symptoms
Here’s the key insight: While this is an anatomical quirk that some people are born with, there still needs to be an activating event.
In Long COVID and Post-Vaccine Syndrome patients, spike protein is actively causing this problem through two main pathologies that impact the structural integrity of blood vessel walls.
— Clinical Observation from Leading Edge Clinic:
In our practice, we’ve observed that many Long COVID and Post-Vaccine Syndrome patients present with venous compression that wouldn’t have been clinically significant before spike protein exposure. The spike-induced endothelial and collagen dysfunction appears to transform anatomical variations that were previously asymptomatic into symptomatic compression syndromes.
One representative case: A 34-year-old female developed severe POTS 6 months post-vaccination. Imaging revealed 60% left common iliac vein compression—a finding that may have been present anatomically for years but only became symptomatic after spike protein triggered endothelial dysfunction and reduced her venous compliance.
Another case: A 30 year old male had a gradual onset of POTS that eventually became severe post-vaccination. Prior to Post-Vaccine Syndrome, patient was active, working out 6 days a week (hot yoga, kettlebell HIIT workouts, 30 mile cycling rides, etc…). A 3 day treatment of stem-cell exosomes improved some chest pain symptoms, but the POTS symptoms remained. Patient found mornings to be particularly difficult, with leg pain upon waking. Minor exertion caused continued chest pain and poor recovery. MRA and MRV revealed a significant stenosis indictative of IVC, which was confirmed by Dr. Brooke Spencer during an IVUS at stenting procedure. The IVUS showed an 80+% stenosis. POTS symptoms resolved upon stenting.
From the clinical observations of Dr. Scott Marsland, practice partner at Leading Edge Clinic —
The Spike Protein Connection
Why do so many Long COVID and Post-Vaccine Syndrome patients develop venous compression?
Two mechanisms:
1. Endothelial Dysfunction
Spike protein damages the endothelium (the inner lining of blood vessels), especially the glycocalyx. This causes:
Inflammation of vessel walls
Reduced elasticity
Impaired vascular function
Makes veins more susceptible to compression
Your veins rely on healthy endothelium to maintain their structure and resist external pressure. When spike protein damages this lining, the veins become weaker and more easily compressed.
2. Collagen Dysfunction
Spike protein also interferes with normal collagen synthesis and function. This creates a situation similar to what we see in Ehlers-Danlos Syndrome (EDS):
Weakened connective tissue
Reduced structural support for veins
Increased vein distensibility (they stretch and collapse more easily)
Higher risk of venous compression syndromes
Think about it like this: If the walls of your vein are weakened by spike-induced collagen dysfunction, they’re more likely to collapse under the pressure of the artery sitting on top.
This is why we see such high rates of venous compression in Long COVID and Post-Vaccine Syndrome patients compared to the general population. Before spike protein was in our environment, symptomatic iliac venous compression was triggered by acute traumatic events, such as childbirth in women. Or, in chronic conditions that are less prevalent, less virulent, than Long Covid and Post-Vaccine Syndrome (ie: Lymes disease).
What We’re Seeing in Practice
After evaluating hundreds of Long COVID and Post-Vaccine Syndrome patients with POTS, we’ve identified consistent patterns:
Collagen dysfunction markers:
Patients who previously had no hypermobility now showing joint laxity
The pattern we see: Patients with more severe endothelial and collagen dysfunction tend to have worse venous compression, even with similar anatomical compression ratios.
This suggests spike protein damage intensity determines symptom severity more than degree of anatomical compression alone.
How This Causes POTS: The Vicious Cycle
Here’s how iliac venous compression drives POTS symptoms:
Standing up triggers a cascade:
Gravity pulls blood down to your legs
Your compressed iliac vein can’t efficiently return blood to your heart
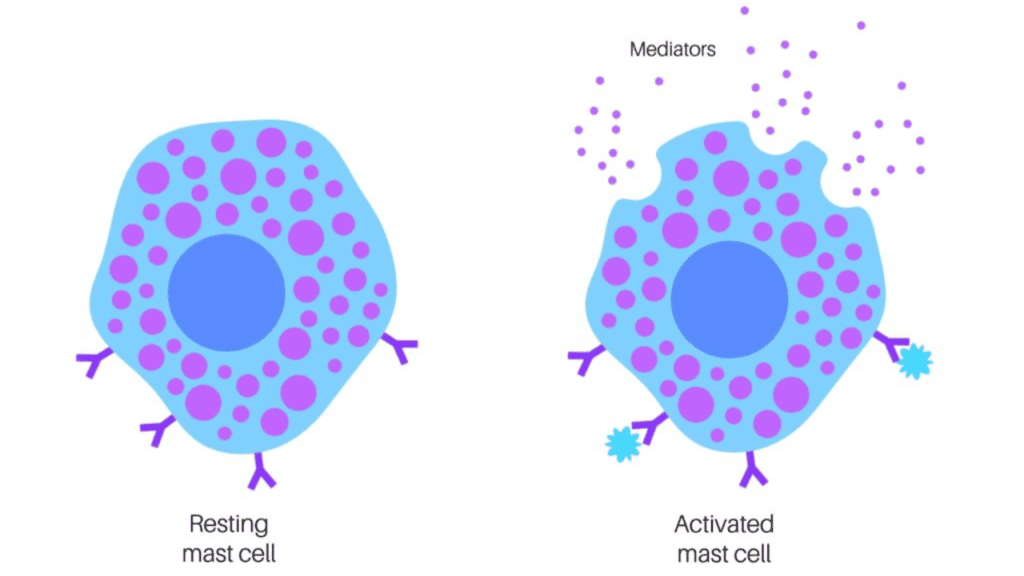
Mast cell mediators → more inflammation, more vascular dysfunction
Worse vascular function → more venous compression
Round and round it goes
Why This Matters for Treatment
If you treat MCAS but ignore venous compression:
Antihistamines and mast cell stabilizers help temporarily
But the underlying trigger (venous congestion) persists
MCAS keeps flaring despite medication
“I’m on 6 different MCAS medications and still symptomatic”
If you treat venous compression:
Improved venous drainage reduces tissue hypoxia
Better circulation clears inflammatory mediators
Less mast cell triggering
MCAS symptoms often improve significantly
Some patients need fewer MCAS medications
This is why so many patients have the “POTS-MCAS-EDS trifecta.” The mechanisms overlap and reinforce each other. Treating venous compression addresses a root cause that’s driving both conditions.
Why Standard POTS Treatments Don’t Work for Venous Compression
Let’s look at why the usual approaches fall short when venous compression is the underlying issue:
Salt and Hydration
Standard advice: Increase salt and fluid intake to expand blood volume.
Why it doesn’t fully work: You’re expanding the volume, but the venous “highway” is still blocked. The blood still can’t get back to your heart efficiently. You might get minor improvement, but you’re not addressing the structural obstruction.
Our experience: Patients often say “I’m drinking so much water and salt I feel bloated, but I’m still symptomatic.”
Compression Stockings
Standard advice: Wear compression stockings to reduce venous pooling in the legs.
Why it doesn’t fully work: Compression stockings help prevent blood from pooling in the lower leg veins. But if the iliac vein is compressed, blood still can’t get past that obstruction to reach the heart. You’re compressing the bottom of the system while the top is blocked.
Our experience: “The stockings help a little, but I still crash after standing for 15 minutes.”
Beta-Blockers and Midodrine
Standard advice: Beta-blockers to slow heart rate, midodrine to constrict blood vessels and raise blood pressure.
Why it doesn’t fully work: These are symptomatic treatments. They’re addressing the compensatory response (fast heart rate, low blood pressure) but not the root cause (poor venous return).
Our experience: “The medication keeps my heart rate from going as high, but I still feel awful when I stand.”
Exercise Reconditioning
Standard advice: Gradual exercise to recondition the autonomic nervous system.
Why it doesn’t fully work: If your venous return is structurally impaired, exercise can actually make things worse. You’re asking a compromised system to do more work.
Our experience: “Every time I try to exercise, I crash for days afterward.”
How to Know If Venous Compression Is Driving Your POTS
Red flag symptoms that suggest venous insufficiency:
Left leg symptoms more than right
Swelling, heaviness, discomfort primarily in left leg
Visible varicose veins or spider veins on left leg
Left leg feels “tired” or “heavy” by end of day
Not a guarantee; some patients bilateral symptom burden is equal
Pelvic symptoms
Pelvic pain or pressure (especially in women)
Pain that worsens with prolonged standing
Relief when lying down with legs elevated
Worse in the morning
Visible bloating
Skin changes
Red or purplish-brown discoloration on legs
Hemosiderin deposits (brownish staining from old blood)
Visible venous pooling when standing
Positional worsening
POTS symptoms dramatically worse after standing/sitting for extended periods
Significant improvement when legs are elevated
“I feel best lying down with my feet up”
Post-exertional crashes
Walking, standing, or light activity triggers severe crashes
Recovery takes days, not hours
Exercise intolerance seems disproportionate to deconditioning
Mast Cell Activation Symptoms – Flushing episodes, especially in legs or pelvis, but can be systemic – Hives or skin reactions that worsen with standing – Abdominal pain, bloating, or digestive issues (pelvic venous congestion affecting GI tract with some experiencing IBS) – Histamine intolerance symptoms that correlate with POTS flares – “I have both POTS and MCAS and they seem to trigger each other”
Worsening MCAS with Venous Symptoms – MCAS flares worsen in the morning (as venous pooling worsens overnight) – Flushing and hives worse in the evenings – Antihistamines help MCAS but don’t touch the POTS – “My mast cell symptoms are worse when my legs are swollen”
We have even seen some patients developing autoimmune conditions of the CNS. After undergoing interventions for Iliac Venous Compression, these patients saw symptoms related to these conditions going into remission. This is a clinical observation, and more study is required to understand the link between venous compression, pelvic blood stasis, and CNS autoimmunity.
If you have several of these, venous compression should absolutely be evaluated.
Diagnostic Testing for Venous Compression
If we suspect venous compression based on symptoms, here’s how we evaluate:
Gold Standard: MRI Venography & MRI Angiography
Detailed view of pelvic vasculature
Visualizes the iliac veins and arteries, and extent of compression
Can identify May-Thurner Syndrome, Nutcracker Syndrome, pelvic congestion
Best non-invasive diagnostic tool
Based on our work with Dr. Brooke Spencer, and Interventional Radiologist with decades of experience treating Iliac Venous Compression, her specific MRV and MRA protocol that we use is the only way to identify Iliac Venous Compressions that do not involve a Deep Vein Thrombosis.
Most Definitive: Intravascular Ultrasound (IVUS)
Performed during venography
Provides detailed assessment from inside the vein
Can measure exact degree of compression
Often done if stenting is being considered
Our approach: We typically start with symptoms and clinical examination. If venous compression is suspected, we refer for appropriate imaging. The key is working with vascular specialists who understand the POTS connection, such as Dr. Brooke Spencer.
Treatment Approaches for Venous Compression in POTS
When we identify venous compression as a driver of POTS, we have several treatment options:
Conservative/Medical Management
For mild to moderate compression, we start with:
1. Flavay (Oligomeric Proanthocyanidins)
Supports vascular health and collagen integrity.
Strengthens blood vessel walls
Reduces inflammation
Improves venous tone
Supports endothelial function
Additional benefit for MCAS patients: Flavay (OPCs) also has mast cell stabilizing properties. By supporting vascular integrity AND stabilizing mast cells, it addresses both the venous compression and the MCAS component simultaneously.
Why it works for spike protein damage: Helps repair the collagen and endothelial dysfunction caused by spike. Think of it as rebuilding the structural integrity of your veins.
2. Sulodexide
A glycosaminoglycan that improves endothelial function and reduces venous insufficiency.
Restores endothelial barrier function
Reduces inflammation in vessel walls
Improves blood flow
Decades of use for chronic venous insufficiency in diabetic patients in the EU
Why this also matters for MCAS: By restoring endothelial function and improving venous drainage, sulodexide reduces the hypoxic and inflammatory triggers that cause mast cell degranulation. Many patients report improvement in both POTS and MCAS symptoms.
Why it works for Long COVID/PVS: Directly addresses the endothelial dysfunction caused by spike protein. Fast-moving heparin penetrates the endothelium at a deeper level, reaching and healing the glycocalyx. Multiple studies show improvement in venous function.
Typical protocol: Usually combined with other interventions targeting spike protein clearance and vascular repair. Treatment duration varies. It is very important to note that the underlying spike protein pathology needs to be addressed. The endothelial impacts are systemic, and will cause other future conditions. However, Iliac Venous Compression is a significant and serious bottleneck deserving of immediate attention.
3. Softwave Therapy
Regenerative therapy that promotes tissue healing.
Stimulates collagen production
Improves blood flow
Reduces inflammation
Promotes vascular regeneration
Why it works: Helps rebuild the damaged connective tissue and vascular structures affected by spike protein. There are already sexual health clinics that have used Softwave Therapy for many years to help male patients with Erectile Dysfunction, indicating the efficacy of healing the vasculature.
Interventional Treatment: Venous Stenting
For moderate to severe compression that doesn’t respond adequately to conservative treatment:
What it is: Minimally invasive procedure where a balloon widens the compressed vein, then a stent is permanently placed to hold it open and restore normal blood flow.
Success rates: Research shows significant symptom improvement in POTS patients after iliac vein stenting:
83% of POTS patients** have confirmed venous compression on imaging (eClinicalMedicine, 2026)
Significant quality of life improvements** at 3 and 12 months post-stenting, with improvements in physical functioning (+19 points), energy/fatigue (+13 points), pain (+10 points), and social function (+26 points) (JACC, 2024)
97.1% stent patency** at 3 years for non-thrombotic iliac vein compression (the type POTS patients have) – the best outcomes of all venous stenting groups (ABRE study, 2021)
90-95% long-term patency rates** across multiple large studies
Low complication rates:** 1.7% major bleeding, 0% stent fractures in dedicated venous stents
At Leading Edge Clinic, our observations have mirrored what was found in these studies, with some caveats. Because Long Covid and Post-Vaccine Syndrome are complex, multi-system conditions, there is other intervention required for ongoing health. However, our patients nearly always see a significant improvement in POTS symptoms following appropriate intervention for Iliac Venous Compressions. We work with experts like Dr. Brooke Spencer because of her pioneering in the space. Stenting alone requires specialized knowledge of the condition (ie: appropriate stent size for patients).
Important caveat: This is typically done in conjunction with other Long COVID/PVS treatments. Venous compression is often one piece of a multi-system problem.
Why This Is Rarely Diagnosed
You might be wondering: If 50-70% of POTS patients have venous compression, why isn’t this being diagnosed more often?
Several reasons:
1. Most Doctors Aren’t Looking for It
Standard POTS evaluation focuses on:
Tilt table test
Autonomic testing
Heart rate and blood pressure monitoring
Pelvic venous imaging isn’t part of the typical POTS work-up. Unless you’re seeing a vascular specialist, it often gets missed. “Standard of Care” for iliac venous compression is to only look for it, and only treat it if patients are positive for a Deep Vein Thrombosis in the affected area.
2. Symptoms Overlap
The symptoms of venous insufficiency (fatigue, dizziness, exercise intolerance) overlap completely with general POTS symptoms. Without specific venous symptoms (leg swelling, pelvic pain), doctors don’t think to check. Patients can have IVC without leg swelling and pelvic pain.
3. Vascular and Autonomic Specialists Don’t Often Communicate
POTS patients usually see cardiologists or autonomic specialists. Venous compression is diagnosed by vascular surgeons or interventional radiologists. These specialties don’t always talk to each other about the same patient. Furthermore (and to reiterate), many vascular surgeons have been trained to only look for, and intervene on Iliac Venous Compressions if patients develop a Deep Vein Thrombosis in the left common iliac vein.
4. It’s a Relatively New Connection
The research connecting POTS and venous compression has mostly emerged in the last 5-10 years. Many doctors simply aren’t aware of this link yet. Specialists like Dr. Brooke Spencer have been observing this clinically for over two decades, while many of her colleagues have followed standard of care that ignores this connection.
5. Long COVID and PVS Are Making It More Common
The spike protein-induced vascular damage is likely increasing the prevalence beyond what we saw in traditional POTS. We’re seeing this connection more and more in our Long Covid and Post-Vaccine Syndrome patients
Our Comprehensive Treatment Approach
At Leading Edge Clinic, we don’t just treat POTS symptoms. We look for and address the root causes, including venous compression.
Here’s our approach:
Step 1: Comprehensive Evaluation
Detailed symptom history (looking for venous insufficiency clues)
Physical examination
Review of any previous imaging
Assessment for other Long COVID/PVS mechanisms
Step 2: Root Cause Assessment
We evaluate for multiple mechanisms that can drive POTS in Long COVID/PVS:
POTS is rarely one thing. It’s usually multiple dysfunctions working together.
Step 3: Multi-Targeted Treatment
If venous compression is present:
Start with vascular support (Flavay, Sulodexide)
Consider Softwave therapy
Refer to interventional radiology or vascular specialist if imaging shows significant compression
Coordinate care if stenting is pursued
Simultaneously address:
Spike protein clearance
Endothelial repair
Immune modulation (if autoantibodies present)
Mitochondrial support
Autonomic retraining
Mast cell stabilization (especially important if venous compression is triggering MCAS)
Plus conventional POTS support:
Salt and hydration (still helpful even if not the primary solution)
Compression (can help lower leg pooling)
Medication if needed for symptom control
Gradual reconditioning when ready
Step 4: Monitor and Adjust
Regular follow-ups to assess response
Adjust treatment based on symptom improvement
Coordinate with vascular specialists as needed
Continue addressing underlying Long COVID/PVS mechanisms
What to Expect: Recovery Timeline
If venous compression is a major driver and you get appropriate treatment:
Weeks 1-4 (Conservative Treatment)
Start vascular support interventions
May notice reduction in leg heaviness
POTS symptoms still present but potentially less severe
Weeks 4-12
If Flavay/Sulodexide are helping, progressive improvement in venous symptoms
POTS may start improving as venous return improves
Can often begin gentle reconditioning
Months 3-6
Continued improvement in both venous and POTS symptoms
Many patients report being able to tolerate upright posture longer
Exercise tolerance often improves
Some patients ready for interventional options if conservative treatment plateaus
If Stenting Is Performed
Immediate restoration of venous flow
Many patients report rapid improvement in POTS symptoms (within days to weeks), with some improvements taking longer (months)
Continued improvement over months as other mechanisms are addressed
Not a cure-all (you still need to address spike protein, immune issues, etc.), but can be dramatically helpful for the venous component
Key point: If venous compression is your primary POTS driver and it gets treated effectively, improvement can be substantial. But if there are multiple mechanisms (which is common), you need a comprehensive approach.
Clinical Insights from 3,500+ Patients
What predicts treatment success?
Based on our clinical experience, patients who respond best to venous compression treatment share these characteristics:
✓ Younger age (under 50) – better vascular remodeling capacity; though this does not mean patients above 50 do not see significant improvement ✓ Shorter duration of symptoms (under 2 years) – less unchecked vessel damage; again, does not indicate significant improvement is unlikely ✓ Higher baseline function (can stand 10+ minutes) – indicates some compensatory mechanisms intact ✓ Positive response to trial interventions (sulodexide, Flavay) within 4-6 weeks
What makes treatment more challenging?
⚠ Long symptom duration (3+ years) – more fibrotic vessel changes ⚠ Severe autonomic dysfunction (can’t stand at all) – multiple mechanisms involved ⚠ Significant comorbidities (MCAS, EDS, autoimmune) – complexity requires longer treatment ⚠ Ongoing spike protein exposure (repeat infections, ongoing vaccination)
The bottom line: Early intervention yields best results. Waiting 2-3 years while trying ineffective treatments allows more permanent vascular damage.
Why This Matters for Long COVID and Post-Vaccine Syndrome
Standard POTS treatment was developed for idiopathic POTS (POTS without a clear cause).
But Long COVID and Post-Vaccine Syndrome POTS is different. It has specific mechanisms:
Spike protein-induced endothelial damage
Collagen dysfunction
Immune dysregulation
Persistent inflammation
These mechanisms aggressively contribute to venous compression and insufficiency.
This is why generic POTS protocols often fail in Long COVID/PVS patients.
You can’t treat Long COVID POTS the same way you treat traditional POTS. You have to address the spike protein damage, the vascular dysfunction, the immune issues—all of it.
And if you don’t evaluate for and treat venous compression when it’s present, you’re missing a massive piece of the puzzle in 70%+ of patients.
The POTS-MCAS Connection in Long COVID and Post-Vaccine Syndrome
One of the most common patterns we see in Long COVID and Post-Vaccine Syndrome patients:
They develop POTS and MCAS together. This isn’t a coincidence. Here’s why:
Spike Protein Creates the Perfect Storm
Spike protein damages multiple systems simultaneously:
Helps temporarily, but venous compression keeps triggering mast cells
MCAS symptoms return or plateau
If you only treat POTS:
Salt, compression, beta-blockers
Helps some symptoms, but doesn’t address mast cell inflammation
MCAS continues driving vascular dysfunction
If you treat venous compression as part of comprehensive care:
Address structural problem (venous obstruction)
Reduce mast cell triggers (hypoxia, congestion)
Support vascular healing (Flavay, Sulodexide)
Stabilize mast cells simultaneously
Both conditions improve together
This is why our approach addresses all mechanisms simultaneously. You can’t separate POTS from MCAS from venous compression in Long COVID and Post-Vaccine Syndrome patients. They’re interconnected parts of the same spike-driven pathology.
Red Flags You’re Not Getting Proper POTS Care
Be wary if your doctor:
🚩 Never asks about leg symptoms (swelling, heaviness, varicose veins)
🚩 Doesn’t consider venous imaging when standard treatments aren’t working
🚩 Treats your POTS exactly like every other POTS patient (cookie-cutter approach)
🚩 Doesn’t acknowledge the spike protein connection in Long COVID/PVS POTS
🚩 Only offers salt, fluids, and compression stockings without investigating why these aren’t working
🚩 Dismisses your symptoms as “just anxiety” or “deconditioning”
🚩 Doesn’t coordinate with vascular specialists when venous issues are suspected
🚩 Treats POTS and MCAS as separate conditions (doesn’t understand they’re often mechanistically linked)
🚩 Ignores the venous compression-MCAS connection (keeps adding MCAS medications without investigating why mast cells keep degranulating)
What good POTS care looks like:
✓ Comprehensive evaluation including vascular symptoms ✓ Considers multiple mechanisms (not just autonomic dysfunction) ✓ Refers for appropriate imaging when venous compression is suspected ✓ Coordinates care between specialties (interventional radiology, etc…) ✓ Addresses the specific mechanisms of Long COVID/PVS POTS ✓ Combines conventional POTS support with root cause treatment ✓ Regular monitoring and adjustment based on response ✓ Understands the POTS-MCAS connection in Long COVID/PVS ✓ Evaluates for venous compression in patients with treatment-resistant MCAS ✓ Treats the underlying triggers (venous congestion, hypoxia) not just MCAS symptoms
The Bottom Line
If POTS is a significant symptom of your Long Covid or Post-Vaccine Syndrome presentation and standard treatments aren’t working, there’s a very real possibility that venous compression is part of your problem.
This isn’t rare. Research shows 50-70% of POTS patients have significant venous insufficiency. And spike protein damage makes it even more common in Long COVID and Post-Vaccine Syndrome patients.
The good news? When venous compression is identified and treated appropriately, many patients see substantial improvement.
The bad news? Most doctors aren’t checking for this. You may need to advocate for yourself to get proper evaluation.
Next Steps
If you recognize yourself in this article:
If You Haven’t Been Evaluated for Venous Compression
Document your symptoms – especially left leg heaviness, pelvic symptoms, positional worsening
Request vascular imaging – ensure the MRV and MRA follow the Spencer protocol
Find doctors who understand this connection – specialists familiar with POTS, or Long COVID/PVS specialists who coordinate with experts in interventional readiology or vascular care
If You Need Specialized Care
At Leading Edge Clinic, we’ve treated thousands of Long COVID and Post-Vaccine Syndrome patients with POTS. We:
Routinely evaluate for venous compression in our POTS patients
Offer comprehensive treatment addressing all mechanisms (including vascular dysfunction)
Coordinate with vascular specialists when stenting or other interventions are needed
You’ve probably been told your POTS symptoms are “just” autonomic dysfunction. That you need to drink more water, add more salt, exercise more.
But if there’s a compressed vein blocking blood return to your heart, all the salt in the world won’t fix that.
You’re not failing at POTS treatment. The standard approach is failing to identify what’s actually wrong.
Venous compression is real. It’s measurable. It’s treatable.
And when it’s the primary driver of your POTS, addressing it can be life-changing.
You deserve doctors who look for the actual cause, not just treat the symptoms.
You deserve comprehensive evaluation.
And you deserve treatment that works.
Additional Clinical Resources
For deeper dives into specific cases and treatment protocols, Scott Marsland FNP-C (practice partner at Leading Edge Clinic) shares detailed clinical observations on his Substack:
These articles provide the level of clinical detail typically reserved for medical conferences and peer discussions. However, they are not intended as medical advice. Please consult with a qualified medical professional.
References:
Primary POTS-Venos Compression Studies
1. Spencer EB, Saikia J, Ajeya D, Phillips R, Cutchins A, et al. Association and post-iliac vein stenting symptom improvement of postural orthostatic tachycardia syndrome and orthostatic intolerance with pelvic venous disorders: two retrospective studies. eClinicalMedicine. 2026. https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(26)00019-2/fulltext
2. Iliac vein stenting and quality of life in patients with postural orthostatic tachycardia syndrome (POTS). Journal of the American College of Cardiology. 2024. https://www.jacc.org/doi/10.1016/S0735-1097(24)04303-1
3. Brown MT, Pelling MM, Cutchins A, Gilliland CA. Left common iliac vein stenting in a case of postural orthostatic tachycardia syndrome/pelvic pain overlap. Cureus. 2024;16(3):e55974. https://pmc.ncbi.nlm.nih.gov/articles/PMC10927248/
4. Knuttinen MG, Naidu SG, Oklu R, Kriegshauser S, Eversman W, Rotellini L, et al. Imaging findings of pelvic venous insufficiency in patients with postural orthostatic tachycardia syndrome. Clinical Imaging. 2020;64:83-87. https://pubmed.ncbi.nlm.nih.gov/32757696/
5. Ormiston CK, Qadri SK, Gurram N, Singh I, Siddiqui AH. May-Thurner syndrome in patients with postural orthostatic tachycardia syndrome and Ehlers-Danlos syndrome: a case series. European Heart Journal – Case Reports. 2022;6(4):ytac161. https://academic.oup.com/ehjcr/article/6/4/ytac161/6565741
7. Spencer EB, Saikia J, Ajeya D, Phillips R, Cutchins A. Symptomatic improvement in orthostatic intolerance and postural orthostatic tachycardia syndrome and pelvic pain after iliac vein stenting. SSRN. 2025. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5235054
General Venous Stenting Outcomes
8. A meta-analysis of the medium- to long-term outcomes in patients with chronic deep venous disease treated with dedicated venous stents. Journal of Vascular Surgery: Venous and Lymphatic Disorders. 2023. https://www.sciencedirect.com/science/article/pii/S2213333X23004389
9. Final 3-year study outcomes from the evaluation of the Zilver Vena venous stent for the treatment of symptomatic iliofemoral venous outflow obstruction (The VIVO Clinical Study). Journal of Vascular and Interventional Radiology. 2024. https://www.jvir.org/article/S1051-0443(24)00209-4/fulltext
11. Razavi MK, Jaff MR, Miller LE. Safety and effectiveness of stent placement for iliofemoral venous outflow obstruction: systematic review and meta-analysis. Circulation: Cardiovascular Interventions. 2015;8(10):e002772. https://www.ahajournals.org/doi/10.1161/circinterventions.115.002772
12. Ikezawa T, Naiki M, Nakamura M, Ishii H, Kumada Y, Ogino H. Venous stenting for postthrombotic iliocaval venous obstructive disease: clinical efficacy and mid-term outcomes. Annals of Vascular Diseases. 2021;14(2):99-105. https://pmc.ncbi.nlm.nih.gov/articles/PMC9816030/
13. Clinical outcomes at 3 years after stenting for thrombotic and non-thrombotic iliac vein compression syndrome patients. Journal of Interventional Medicine. 2024;7(1):30-38. https://pmc.ncbi.nlm.nih.gov/articles/PMC10787525/
14. Outcomes following iliac vein stenting for non-thrombotic iliac vein lesions—a narrative review based on large sample studies. Life. 2025;16(12):427. https://www.mdpi.com/2079-4983/16/12/427
21. Iliac venous stenting as adjunct in the management of symptomatic orthostatic hypotension in iliac vein compression. Journal of Vascular Surgery Cases, Innovations and Techniques. 2024;10(2):101674. https://www.sciencedirect.com/science/article/pii/S2468428724000674
22. Venous clinical severity score has a suboptimal ability to detect improvement after iliac vein stenting across three years of follow-up. Journal of Vascular Surgery: Venous and Lymphatic Disorders. 2023;11(4):829-838. https://pubmed.ncbi.nlm.nih.gov/36906105/
This article is for informational purposes only and does not constitute medical advice. POTS evaluation and treatment should be undertaken with qualified medical supervision.
About Leading Edge Clinic
We specialize in treating Long COVID, Post-Vaccine Syndrome, POTS, MCAS, and related conditions. Since 2020, we’ve treated thousands of patients nationwide via telehealth, with a focus on identifying and addressing root causes rather than just managing symptoms.
If you’ve been dealing with Post-Vaccine Syndrome for months or even years at this point, you’ve probably already tried a bunch of different treatments. Your medicine cabinet may even be filled with half empty bottles of different supplements.
Maybe you worked through supplement stacks you found in Facebook groups. Maybe you were prescribed antihistamines and told you to “just rest more.” Or you dropped thousands on a functional medicine doc who ran every lab under the sun, handed you a protocol with 30 supplements, and… nothing really changed.
Here’s what we’ve learned after treating over 3,500 patients since 2022:
Most treatments don’t fail because they’re garbage. They may fail for a number of reasons. For instance, treating symptoms instead of fixing what’s actually broken. Most likely, they are failing to sequentially pick up apart the complex multi-system root issues happening with Post-Vaccine Syndrome. It’s like taking Tylenol for a broken bone. Sure, the pain might ease up temporarily, but you still have a broken bone.
In this guide, we are going to walk you through:
Why 70%+ of PVS treatments fail
The 7 biological mechanisms that need to be addressed for real recovery
Why expensive testing usually doesn’t help (and often wastes your money)
What effective treatment actually looks like
How to spot if you’re getting proper care
This isn’t going to be a DIY protocol. PVS is way too complex for that, and honestly, we see patients regularly who’ve made themselves worse with internet treatments. Instead, I this post will focus on what GOOD treatment looks like so you can make informed decisions about your care.
Why Most Post-Vaccine Syndrome Treatments Fail
We’ve evaluated hundreds, probably thousands of patients who tried treatment elsewhere first. Here are the most common reasons their previous treatments didn’t work:
1. Single-Target Approaches
The mistake: Treating PVS like it’s one problem with one solution.
Real example: Patient comes in taking high-dose antihistamines for MCAS symptoms. Gets some relief for 2-3 weeks, then plateaus. The antihistamines are blocking one inflammatory pathway, sure. But they’re not touching the spike protein in your ACE2 receptors, your gut, or your tissue. They also aren’t addressing the microclots, the redox dysfunction, or the nervous system that’s stuck in fight-or-flight mode.
Why it fails: PVS isn’t one thing going wrong. It’s a cascade of interconnected biological dysfunctions. Fix one piece while ignoring the others? The unfixed pieces just keep perpetuating the whole mess.
What we see: Patients spend 6-12 months on single treatments, get minimal improvement, give up thinking “nothing works.”
2. Symptom Suppression Instead of Root Cause Resolution
The mistake: Making symptoms more tolerable rather than fixing what’s broken.
Real example: Patient with crushing fatigue gets prescribed stimulants or high-dose B12. This patient feels more alert for a few hours. But the underlying mitochondrial dysfunction and cellular energy crisis? Still there, getting worse. Within weeks, even the stimulants stop working.
Why it fails: If your mitochondria are damaged, your cells are stuck in emergency mode, or your cells are in a “zombie-like” senescent state, no amount of B vitamins or caffeine is going to restore actual energy. You’re basically whipping an exhausted horse.
The result: Patients become dependent on symptom suppressors that lose effectiveness over time. Meanwhile, the root causes keep getting worse.
3. The “Kitchen Sink” Approach
The mistake: Throwing 20-30 supplements at the problem without any real strategy.
Real example: Patient brings us a list of 35 supplements they’re taking. Everything from vitamin D to exotic mushroom extracts. Total monthly cost: $800. Improvement: basically none.
Why it fails: More isn’t better. Here’s what usually happens with these massive supplement stacks:
Overlapping mechanisms (you’re triple-dosing the same pathway)
Some contradict each other (promoting inflammation while trying to suppress it)
Not targeting YOUR specific problems
Wrong dosing or wrong form
Side effects that mask whether anything’s actually working
What happens: Patients waste thousands of dollars, can’t tell what’s helping versus hurting, and often develop new symptoms from supplement interactions.
4. Chasing Lab Values Instead of Treating the Patient
The mistake: Believing expensive testing will reveal the “one thing” you need to fix.
Real example: Patient spends $5,000 on comprehensive panels. Micronutrient testing, heavy metals, genetics, specialized immune panels, food sensitivities. Gets back a 40-page report with 50 things flagged in red.
Why it fails: Here’s what we’ve learned after treating thousands of patients:
Most PVS patients have completely normal standard labs (that’s part of why doctors dismiss them)
A lot of specialized tests show “abnormalities” that aren’t actually relevant to PVS
Test results often don’t change what we’d do anyway
The most important information comes from your symptoms and how your body responds to treatment
We already know the root causes. We don’t need $5,000 in labs to confirm them.
The reality: We’ve successfully treated thousands of patients without extensive lab work. Your money is better spent on actual treatment.
5. Stopping Treatment Too Early
The mistake: Expecting quick fixes for a complex, chronic condition.
Real example: Patient starts treatment, feels 20% better after 4 weeks, stops because they expected to be “cured” by now. Within 2-3 weeks, they’re back where they started. Or worse.
Why it fails: PVS didn’t develop overnight. It’s not going to resolve overnight either. The biological dysfunctions we’re addressing (spike protein persistence, microclots, cellular danger response, senescent cell burden) take months to fully correct.
An Example of a realistic timeline:
Weeks 1-12: Inflammatory reduction, some symptoms improve
Months 3-12: Steady improvement as root causes get addressed
Year 1+: Major improvements, good days outnumber bad days
Year 1.5+: Continued recovery, return to near-normal function
Year 2+: Maintenance and full recovery for most patients
What we see: Patients who commit to 6-12 months of treatment? 80-85% success rate. Those who stop at 4-8 weeks? 0-5% success rate.
6. Treating PVS Like It’s Something Else
The mistake: Using protocols designed for ME/CFS, Lyme, or MCAS without modification.
Real example: Patient with PVS gets treated with a Lyme protocol. There’s overlap, absolutely. But, PVS has unique features like persistent spike protein, and significant senescent cell burden that require specific interventions. The Lyme approach misses critical pieces.
Why it fails: While PVS shares features with other post-viral conditions, it has distinct mechanisms that must be addressed. Cookie-cutter protocols from other conditions miss what makes PVS different.
The 7 Root Causes That Must Be Addressed
After treating 3,500+ patients, we’ve repeatedly witnessed (not just read the research) seven core biological dysfunctions driving Post-Vaccine Syndrome. You need to address ALL of them. Not just one or two. And, you need to address them sequentially in a manner that makes sense.
1. Persistent Spike Protein
What’s happening: In PVS patients, vaccine-generated spike protein has been detected circulating for 6+ months. Some studies show 700+ days post-vaccination. And what about in the tissues? We know through our work with leading researchers that the spike protein uses commensal gut bacteria to hide out and act as bacteriophages. We have long known that spike protein has an affinity for ACE2 receptors to access cells. We know from post-mortem tissue staining that it is often lodged in organs and other types of tissue.
Why it matters: Spike protein isn’t just sitting there doing nothing. It’s biologically active—triggering ongoing inflammation, damaging blood vessel walls, promoting clotting, keeping your immune system in a constant state of activation, promoting a cell danger response and senescent cell signaling.
Treatment principle: Clear the persistent spike through multiple mechanisms. This isn’t a single medication. It requires a strategic combination targeting different clearance pathways.
What makes this complex:
Spike protein “hides” in different tissues
Clearance rate varies wildly between individuals
Spike will alternate between gut, and systemic locations to hide out
Some products identified for spike protein clearance can actually make the problem worse
Different approaches depending on where spike is concentrated
Depending on burden, can take 3-12+ months to fully clear
Why you can’t DIY this: The agents that clear spike protein also affect clotting. Too aggressive? Bleeding risk. Not aggressive enough? Persistent inflammation. Requires medical judgment and monitoring.
2. Microclot Formation and Vascular Dysfunction
What’s happening: Research shows PVS patients often have microclots. Tiny clots that don’t show up on standard imaging but block blood flow in small vessels. This reduces oxygen delivery to tissues. Result? Fatigue, brain fog, exercise intolerance, and more.
Why it matters: Your cells can’t function without oxygen and nutrients. Microclots create chronic tissue hypoxia (low oxygen), which perpetuates all the other dysfunctions.
Treatment principle: Break up existing microclots, prevent new formation, restore healthy endothelial function.
What makes this complex:
Must assess bleeding risk (some patients can’t tolerate aggressive clot-busting)
Different agents target different clot components
Has to be coordinated with spike protein clearance (they’re related)
Endothelial repair takes months
Over-aggressive treatment causes its own problems (just like over-aggressive spike clearance)
Why you can’t DIY this: Anticoagulation and clot-busting agents are powerful. This needs medical supervision.
3. Chronic Cell Danger Response (CDR)
What’s happening: When cells sense a threat, they enter a protective “cell danger response.” They shut down normal functions, stop making energy efficiently, focus on survival. In PVS, cells get STUCK in this state even after the threat is gone.
Why it matters: Cells in CDR can’t do their jobs. Muscle cells can’t contract efficiently (hello, exercise intolerance). Brain cells can’t communicate well (brain fog). Immune cells malfunction. It’s like your whole body stuck in permanent emergency mode. Or, “battery saver” mode.
Treatment principle: Signal to cells that it’s safe to exit emergency mode and return to normal function. This involves addressing inflammation, restoring cellular energy production, calming danger signals.
What makes this complex:
CDR is protective. You can’t just “turn it off”
Requires creating conditions where cells feel safe to exit
Different tissue types respond to different signals
Must be addressed systematically
Takes time. Cells don’t trust the “all clear” signal immediately
Why you can’t DIY this: Exiting CDR requires strategic sequencing. Push too hard too fast? Cells retreat deeper into defense mode. Requires clinical experience.
4. Redox Imbalance and Oxidative Stress
What’s happening: Your cells use controlled oxidation to generate energy and fight infections. But in PVS, the redox system gets thrown out of balance. Too much oxidative stress, not enough antioxidant capacity. Cells are essentially rusting from the inside.
Why it matters: Excessive oxidative stress damages mitochondria (your cellular power plants), creates inflammation, damages DNA, impairs every cellular process. It’s a major driver of fatigue, brain fog, and tissue damage.
Treatment principle: Restore redox balance. Not by flooding the system with antioxidants (which often doesn’t work), but by repairing the cellular mechanisms that regulate oxidation and reduction.
What makes this complex:
Too many antioxidants can actually make things worse (yes, really)
Different tissues need different redox approaches
Must support mitochondrial function simultaneously
Redox dysfunction and CDR feed into each other—must address both
Requires specific nutrients and cofactors in precise forms
Why you can’t DIY this: The supplement industry sells “antioxidants” as a cure-all. In reality, crude antioxidant supplementation often fails in PVS because it doesn’t address the underlying regulatory dysfunction. Can even cause harm by disrupting what little redox balance remains.
5. Autonomic Nervous System Dysregulation
What’s happening: Your autonomic nervous system (ANS) controls automatic functions like heart rate, blood pressure, digestion, temperature regulation. In PVS, the ANS gets stuck in “fight or flight” mode or swings wildly between sympathetic and parasympathetic states.
Why it matters: ANS dysfunction causes POTS, blood pressure instability, temperature problems, digestive issues, and worsens every other symptom. Plus it’s self-perpetuating—ANS dysfunction increases inflammation and oxidative stress, which worsens ANS dysfunction.
Treatment principle: Calm the nervous system, restore autonomic balance, retrain the ANS to function normally. This involves both top-down (nervous system) and bottom-up (reducing inflammatory signals) approaches.
What makes this complex:
ANS dysfunction has multiple causes in PVS (inflammation, redox dysfunction, microclots affecting brain blood flow, vagus nerve damage)
Must address root causes while providing symptomatic support
Different patients need sympathetic suppression versus parasympathetic activation
Timing matters. Push ANS retraining too hard and symptoms worsen
Requires months of consistent intervention
Why you can’t DIY this: Many patients try beta-blockers or other meds for POTS and get minimal relief. Why? Because they’re not addressing WHY the ANS is malfunctioning. Effective treatment requires understanding how ANS interacts with the other six dysfunctions.
6. Immune Dysregulation
What’s happening: Healthy immune function recognizes threats, mounts appropriate response, returns to baseline. In PVS? The immune system becomes chronically dysregulated. It’s simultaneously overactive (attacking your own tissues) and underactive (failing to clear threats properly). Elevated inflammatory cytokines like IL-6 and IL-8, autoantibody formation, T-cell exhaustion, impaired immune surveillance.
Why it matters: Immune dysregulation perpetuates inflammation even after the initial trigger (vaccination) is long gone. It drives tissue damage, prevents healing, worsens fatigue, creates a vicious cycle where the immune system itself becomes part of the problem. This is also why some PVS patients develop new autoimmune symptoms or reactivation of latent viruses like EBV or HHV-6.
Treatment principle: Rebalance immune function. Not by simply suppressing it (creates other problems) or stimulating it (can worsen autoimmunity), but by restoring normal immune regulation. This involves reducing inappropriate inflammatory responses while supporting proper immune surveillance and tolerance.
What makes this complex:
The immune system has multiple arms (innate, adaptive, cellular, humoral) that can be dysregulated in different ways
Some patients need immune modulation, others need support, many need both
Autoantibodies may be targeting specific receptors (adrenergic, muscarinic, etc.) requiring targeted approaches
Timing matters—aggressive immune intervention too early can worsen inflammation
Must address other root causes simultaneously (spike protein drives immune activation, CDR affects immune cell function)
Reactivated viruses (if present) must be addressed or immune rebalancing fails
Why you can’t DIY this: Immune modulation isn’t something you do with random supplements. We’ve seen patients get significantly worse from inappropriate immune stimulation (making autoimmunity worse) or excessive suppression (leading to infections, viral reactivation). Requires understanding which aspects of immune function are overactive versus underactive in YOUR specific case.
7. Senescent Cell Accumulation
What’s happening: When cells are damaged beyond repair, they’re supposed to either die (apoptosis) or get cleared by the immune system. In PVS, damaged cells often become “senescent.” They don’t die, but they don’t function either. Worse, they secrete inflammatory signals that damage surrounding healthy cells.
Why it matters: Senescent cells are zombie cells. Not alive, not dead, but toxic to everything around them. They accelerate aging, promote inflammation, prevent tissue healing. Accumulation of senescent cells is why PVS patients often feel like they “aged overnight.”
Treatment principle: Selectively eliminate senescent cells (senolysis) while preventing new senescent cell formation. This allows tissues to regenerate with healthy cells.
What makes this complex:
Senolytics (agents that clear senescent cells) can’t be used continuously
Must be pulsed strategically to avoid side effects
Different senolytics target different cell types
Timing matters—too early and too aggressive in treatment can worsen inflammation temporarily
Must be balanced with supporting healthy cell regeneration
Why you can’t DIY this: Natural senolytics (like quercetin) get marketed heavily online, but they’re weak and often ineffective at meaningful doses. Stronger senolytics have side effects and timing considerations that require medical guidance.
Why All Seven Must Be Addressed Simultaneously
Here’s the thing: These seven dysfunctions feed into each other.
For example:
Persistent spike protein → creates oxidative stress and inflammation → triggers immune dysregulation
Immune dysregulation → produces inflammatory cytokines and autoantibodies
Autoantibodies → worsen ANS dysfunction (if targeting adrenergic/muscarinic receptors)
ANS dysfunction → increases inflammation → increased inflammation increases risk of microclotting
This is why single-target treatments fail. You might temporarily suppress one piece, but the other six keep driving the system back into dysfunction.
Effective treatment has to:
Address all seven mechanisms
Do it in a coordinated, sequential way (not random supplements)
Use agents that target multiple mechanisms where possible
Be sustained long enough for the positive feedback loops to reverse
Get adjusted based on how you respond
This is also why PVS treatment can’t be cookie-cutter. Your dominant dysfunction might be microclots and immune dysregulation. Another patient’s might be CDR and redox imbalance. Another’s might be ANS dysfunction and senescent cells. The framework is the same, but the emphasis and sequencing has to be personalized.
Why Expensive Testing Usually Isn’t Necessary
One of the most common questions: “What labs should I run before starting treatment?”
Honest answer: Probably fewer than you think.
What We’ve Learned About Testing in PVS
After treating thousands of patients:
Standard labs are usually normal in PVS
CBC, CMP, thyroid, and inflammatory marker are either stypically unremarkable, or can jump all over the place depending on the day (highlighting the dysfunction)
Normal labs result in conventional doctors dismissing PVS patients (“your labs are fine”)
Yeah, we could measure your IL-6, IL-8, spike protein levels, autoantibodies
But we already know these are likely dysregulated—you have PVS
The treatment approach is the same whether your IL-6 is 3x or 5x elevated
These tests cost $500-$2,000 and usually don’t alter the plan
The most important information comes from clinical evaluation
Your symptom pattern tells us which mechanisms are dominant
Your response to initial treatment guides adjustments
Your exercise tolerance, POTS symptoms, cognitive function. These are your biomarkers
We can clinically assess what’s happening without expensive labs
Testing can actually delay treatment
Patients spend $3,000-$5,000 on comprehensive panels
Wait 2-3 weeks for results
Get overwhelmed by the data
Delay starting treatment by a month or more
That’s a month of continued suffering for information that rarely changes the plan
When We Do Recommend Testing
Look, we’re not anti-testing. We just believe testing should be strategic, not reflexive.
We might recommend basic labs if:
You haven’t had recent standard work-up (CBC, CMP, thyroid) to rule out other stuff
You have specific risk factors that need assessment (anemia, kidney function, etc.)
You’re considering treatments that require baseline values
We might recommend specialized testing if:
Your presentation is atypical and we’re considering alternative diagnoses
You’re not responding to treatment as expected after 2-3 months
You have insurance that covers advanced testing at no cost to you
But for most PVS patients: We know the problem. We know the root causes. We know what needs to be addressed. Let’s start treatment and see how you respond. That gives us more useful information than any lab panel.
The Money Argument
Option A: Spend $4,000 on testing
Comprehensive panels
Wait for results
Start treatment 4-6 weeks later
Treatment costs $300-500/month
Total first 3 months: $5,900
Option B: Skip unnecessary testing
Basic screening only ($200-400 if not covered)
Start treatment immediately
Adjust based on how you respond
Treatment costs $300-500/month
Total first 3 months: $1,600
You save $3,000-4,000 AND start treatment a month sooner.
Where would that money be better spent? On the actual treatments that make you better.
What Effective Treatment Actually Looks Like
Now that you understand what doesn’t work and what root causes must be addressed, let’s talk about what good PVS treatment actually looks like.
Note: This is NOT a DIY protocol. I’m describing the framework and principles, not specific drugs or doses. PVS treatment must be medically supervised.
The Treatment Framework
Phase 1: Foundation and Stabilization (Weeks 1-12)
Goals:
Reduce acute inflammation
Stabilize autonomic symptoms
Balance redox pathways
Gently begin spike protein clearance
Establish baseline for monitoring progress
What happens:
You start with a core set of interventions targeting multiple mechanisms
Dosing is usually conservative initially to assess tolerance
We monitor for side effects and early response
Adjustments based on your specific symptom pattern
What to expect:
Some patients feel worse before better (Herxheimer-like reaction from spike clearance)
Energy might be unstable—good days and bad days
Sleep often improves first
Exercise tolerance usually hasn’t improved yet (too early)
Brain fog may start to lift slightly
Phase 2: Root Cause Resolution (Months 3-9)
Goals:
Ttirate up spike protein clearance
Break up microclots and restore microcirculation
Continue redox balance restoration
Begin ently guiding cells out of danger response
Rebalance immune function and address autoimmunity
Gently begin clearing senescent cells (pulsed approach)
Continue retraining autonomic nervous system through different stage
What happens:
Treatment intensifies based on your response
We sequence interventions strategically (some things must happen before others)
Different mechanisms get emphasized based on what’s improving versus what’s stuck
Monthly check-ins to assess progress and adjust
What to expect:
Steady improvement—each month notably better than the last
Good days start to outnumber bad days
Exercise tolerance begins improving (slowly)
Brain fog clears significantly
Fatigue reduces
Autonomic symptoms stabilize
Occasional setbacks (normal, not linear)
Phase 3: Optimization and Maintenance (Months 9-18+)
Goals:
Complete spike protein clearance
Continue building mitochondrial capacity appropriately
Begin rebuilding exercise capacity if ready
Achieve stable autonomic function
More aggressive senescent cell clearance and CDR therapy
Transition to maintenance approach
What happens:
Focus shifts from correction to optimization
We start weaning interventions that are no longer needed
Emphasis on supporting lasting recovery
What to expect:
You feel like yourself again (or close)
Energy is consistent
Can exercise without crashes
Brain fog is minimal to gone
Most days feel “normal”
Occasional mild symptoms but manageable
Key Principles of Effective Treatment
Multi-targeted, not single-agent Every intervention targets multiple dysfunctions where possible. Creates synergistic effects rather than isolated improvements.
Strategic sequencing Some interventions must come before others. Aggressively pushing mitochondrial support before addressing CDR often fails—cells won’t respond while still in danger mode. Similarly, immune modulation must be timed appropriately.
Individualized emphasis The framework is the same for all patients, but emphasis varies. If your dominant issue is POTS with adrenergic autoantibodies, we emphasize ANS, immune modulation, and microvascular interventions. We will look for an iliac venous compression to see if venous return flow is causing your POTS. If it’s crushing fatigue with immune exhaustion, we emphasize mitochondrial, redox support, and immune rebalancing.
Clinical monitoring over lab monitoring We track what matters: How’s your energy? Can you exercise? How’s your brain fog? How often do you crash? These clinical markers guide treatment better than lab values.
Patience and persistence Recovery takes 12+ months for most patients. We see the best outcomes in patients who commit to the full process rather than expecting quick fixes.
Avoiding common pitfalls We actively prevent the mistakes described earlier—no single-target approaches, no symptom suppression without addressing root causes, no premature discontinuation.
Red Flags: How to Know if You’re Getting Poor Care
Not all doctors treating PVS are equal. Here are warning signs you might not be getting good care:
Red Flag #1: They Want $5,000+ in Testing Before Starting Treatment
Why this is a problem: As discussed, extensive testing rarely changes the treatment approach. This is often more about the provider’s revenue model than medical necessity.
What good care looks like: Basic screening if needed, then start treatment. Let your response guide decisions.
Red Flag #2: They Give You a 30-Supplement Protocol on Day One
Why this is a problem: Random supplement stacks aren’t strategic. You can’t tell what’s helping, what’s hurting, what’s unnecessary. Usually based on what the provider sells.
What good care looks like: Focused, strategic approach targeting specific mechanisms. You should understand WHY you’re taking each thing.
Red Flag #3: They Promise Quick Results
Why this is a problem: Anyone promising you’ll be “cured in 4-6 weeks” doesn’t understand PVS. This is a chronic condition requiring months of treatment.
What good care looks like: Honest expectations—some improvement in 4-8 weeks, steady improvement in 3-9 months, major in 9-18+ months for most patients.
Red Flag #4: They’re Using a Cookie-Cutter Protocol
Why this is a problem: “I use the same protocol for everyone” means they’re not actually treating YOUR specific presentation.
What good care looks like: A framework that applies to all PVS patients, but with individualized emphasis and adjustments based on your specific dysfunctions and response.
Red Flag #5: They Can’t Explain the Mechanism
Why this is a problem: If your provider can’t explain WHY you’re taking something and WHAT mechanism it’s targeting, they probably don’t have a strategic framework.
What good care looks like: You should understand the treatment rationale. Good providers can explain in plain language what each intervention does and which dysfunction it addresses.
Red Flag #6: No Follow-Up or Adjustment Plan
Why this is a problem: “Call us if you have problems” isn’t a treatment plan. PVS requires regular monitoring and adjustment.
What good care looks like: Regular check-ins (usually bi-weekly in early stages), systematic assessment of progress, adjustments based on your response.
Red Flag #7: They’re Only Treating Symptoms
Why this is a problem: If all they’re offering is antihistamines for POTS, beta-blockers for heart rate, sleep aids for insomnia—they’re not addressing root causes.
What good care looks like: Symptomatic support is fine as part of comprehensive treatment, but the focus should be on resolving the underlying dysfunctions.
Why Treatment Fails Even with Good Care
Even with proper treatment, some patients don’t improve as expected. Most common reasons:
1. Ongoing Exposure or Reinjury
The problem: Continued COVID infections, additional vaccinations, or other immune triggers keep reactivating the dysfunctions you’re trying to resolve.
What happens: You improve for a few weeks, then relapse. Treatment seems to work briefly then stops. Ongoing senescent cell burden for repeat exposures is a big underlying cause
The solution: Avoiding reinjury is critical during recovery. Doesn’t mean living in a bubble, but being strategic about risk.
2. Unaddressed Comorbidities
The problem: Some patients have concurrent conditions (mold illness, Lyme, MCAS, reactivated EBV/HHV-6) that perpetuate inflammation and immune dysregulation even when PVS-specific mechanisms are addressed.
What happens: Partial improvement that plateaus around 50-60% recovery. The immune system can’t fully rebalance because there’s an ongoing trigger (chronic infection, mold exposure) keeping it activated.
The solution: Comprehensive evaluation to identify and address other contributors. For example, if you have high EBV titers from reactivation, addressing that specifically while treating PVS is essential for full recovery.
3. Non-Compliance
The problem: Missing doses, stopping and starting treatments, not following through on the full plan.
What happens: Inconsistent results, minimal improvement, frustration.
The solution: Commit to the full treatment protocol for at least 3-6 months. If cost is the barrier, discuss with your provider. There are often more affordable alternatives.
4. Unrealistic Expectations
The problem: Expecting to feel “100% cured” when you’re actually at 75-80% recovery. Or expecting linear improvement when recovery is typically wavy.
What happens: Discouragement and premature discontinuation despite actually improving.
The solution: Define what “recovery” means to you realistically. For some people, getting from 30% function to 80% function IS success, even if you’re not back to your 25-year-old peak.
Single-target treatments fail because these dysfunctions perpetuate each other You must address all seven in a strategic, coordinated way.
Expensive testing is usually unnecessary We know the root causes. Clinical evaluation and response to treatment provide better information than lab values.
Recovery takes time—usually 12+ months Anyone promising quick fixes doesn’t understand PVS. Commit to the process.
Treatment must be medically supervised This is too complex for DIY. The agents involved have real risks and require professional guidance.
Not all providers treating PVS are equal Look for someone who understands the root mechanisms, has experience treating hundreds of patients, uses a strategic framework rather than random interventions.
Most patients can recover with proper treatment Our success rate with patients who complete 9+ months of comprehensive treatment is 80-85%. This isn’t a hopeless condition.
Next Steps: Getting the Right Care
If you recognize yourself in this article—if you’ve been struggling with PVS and haven’t gotten better with other approaches—it may be time to seek specialized care.
What to Look for in a Provider
Experience matters. Look for providers who’ve treated hundreds (ideally thousands) of PVS patients. This is not a condition where you want to be someone’s first case.
Framework over randomness. The provider should articulate a clear treatment framework based on root cause mechanisms, not just “let’s try this and see.”
Realistic expectations. Be wary of promises of quick cures. Trust providers who are honest about timelines and success rates.
Strategic approach to testing. Good providers don’t reflexively order $5,000 in labs before starting treatment.
Individualization. While the framework should be consistent, application should be personalized to your specific presentation.
What to Expect from Your First Appointment
A good initial evaluation should include:
Comprehensive symptom history
Timeline of symptom onset and progression
Review of treatments already tried
Assessment of which root mechanisms are most dominant in your case
Discussion of treatment framework and what to expect
Clear explanation of therapies, mechanisms, rationale, etc…
Treatment plan you actually understand
How Leading Edge Clinic Can Help
We’ve specialized in treating post-viral and post-vaccine conditions since 2022. We’ve treated over 3,500 patients with Long COVID, Post-Vaccine Syndrome, and related conditions.
Our approach:
Comprehensive treatment targeting all seven root causes
Strategic, individualized protocols
Minimal unnecessary testing
Nationwide telehealth (available in all 50 states)
Monthly monitoring and adjustment
Honest expectations and proven outcomes
What makes us different:
We’ve seen what works and what doesn’t across thousands of patients
We understand the biological mechanisms deeply (spike persistence, immune dysregulation, CDR, redox, microclots, ANS, senescence)
We don’t use cookie-cutter protocols
We focus resources on treatment, not excessive testing
We’re honest about timelines and realistic about outcomes
Ready to Start Your Recovery?
If you’re ready to move beyond failed treatments and address the root causes of your Post-Vaccine Syndrome, we’re here to help.
We know how frustrating and isolating Post-Vaccine Syndrome can be. You’ve probably been dismissed by doctors, doubted by friends and family, left to figure this out on your own.
You’re not imagining your symptoms. You’re not “just anxious.” You’re not “getting old.” And you’re not doomed to feel this way forever.
Post-Vaccine Syndrome is real. It has identifiable biological dysfunctions. And it’s treatable.
Yes, recovery takes time. It requires a strategic approach. And yeah, you need the right medical guidance.
But with proper treatment addressing all seven root causes? Most patients achieve significant recovery. You can be one of them.
You deserve to feel like yourself again. You deserve to be believed. And you deserve proper care.
We’re here when you’re ready.
Disclaimer: This article is for informational purposes only and doesn’t constitute medical advice. Post-Vaccine Syndrome treatment should only be undertaken with qualified medical supervision. Don’t attempt to self-treat based on information in this article.
About Leading Edge Clinic
We specialize in treating post-viral and post-vaccine conditions—Long COVID, Post-Vaccine Syndrome, MCAS, and related disorders. Since 2022, we’ve treated over 3,500 patients nationwide via telehealth. Our approach is based on understanding and addressing the root biological dysfunctions that drive these conditions.
If you’re experiencing persistent, unexplained symptoms that started shortly after your COVID-19 vaccination, you’re not alone, and you’re not imagining it. Post-Vaccine Syndrome (PVS), also called Post-Acute COVID-19 Vaccination Syndrome (PACVS), is an increasingly recognized condition affecting a small percentage of vaccine recipients.
The challenge? Many doctors aren’t familiar with PVS, dismissing symptoms as anxiety or “normal” post-vaccination effects. This leaves patients confused, undiagnosed, and without the specialized care they need.
This guide will help you recognize the warning signs of Post-Vaccine Syndrome, understand how it differs from acute vaccine side effects, and know when to seek specialized medical care.
What Is Post-Vaccine Syndrome?
Post-Vaccine Syndrome is a chronic condition characterized by persistent, multi-system symptoms that develop shortly after COVID-19 vaccination and last for weeks, months, or even years.
According to research from Yale University’s LISTEN Study, PVS patients experience debilitating symptoms that begin within hours to days of vaccination, with a median onset of just three days, and continue long after normal vaccine side effects should have resolved. In our own experience, these symptoms can even develop months after mRNA vaccination, as the condition may also appear through accumulation of spike protein.
The Numbers You Should Know
Symptom onset: Yale study shows typically 1-8 days after vaccination (median: 3 days); but our observations also indicate weeks, to months
Duration: Symptoms lasting 4 weeks or longer (many patients: months to years)
Prevalence: Again, based on Yale data, estimated 0.02-2% of vaccinated individuals; however, we believe this number to be higher based on our patient demographics (70% Post-Vaccine Syndrome versus 30% Long Haul Covid)
Demographics: 80% female, median age 46 years (though it can affect anyone)
Severity: 71-80% of patients report significant impact on daily functioning
Important: PVS is real, recognized by researchers at institutions like Yale, NIH, and leading medical centers. Most importantly, it’s treatable with specialized care.
Understanding the Timeline: When Do PVS Symptoms Start?
One of the most important diagnostic clues for Post-Vaccine Syndrome is when your symptoms began.
Duration: 4+ weeks minimum (often months or years)
Severity: Moderate to severe, often debilitating
Example: A constellation of multi-system symptoms, as opposed to an acute injury
According to the Yale LISTEN Study of 241 PVS patients:
Median symptom onset: 3 days after vaccination
Range: 1-8 days (though some patients report onset within hours)
Duration at time of study: Median 595 days (nearly 20 months)
Why timing matters: A temporal relationship between vaccination and symptom onset, especially when symptoms start within days, is a key diagnostic indicator that helps distinguish PVS from other conditions. While the Yale study looked at patients who experienced PVS symptoms within days, we also know the temporal association can be drawn out months.
The 7 Core Warning Signs of Post-Vaccine Syndrome
If you’re experiencing several of these symptoms that started shortly after vaccination and have lasted more than 4 weeks, you may have Post-Vaccine Syndrome.
Warning Sign #1: Exercise Intolerance (Affects 71% of Patients)
What it looks like:
Unable to perform physical activities you could do easily before vaccination
Severe exhaustion after minimal exertion (walking up stairs, grocery shopping, light housework)
Recovery takes days or weeks, not hours
“Crashes” after activity that leave you bedbound
How it differs from normal fatigue:
Normal post-vaccine fatigue: Tired but can still function; improves with rest and time
PVS exercise intolerance: Disproportionate exhaustion; worsens with activity; doesn’t improve with rest and is ongoing
Real patient example:“I used to go to the gym five days a week. Now I can’t walk to my mailbox without needing to lie down for hours afterward. It’s been 8 months since my booster.”
This is called Post-Exertional Malaise (PEM) and is one of the hallmark features of PVS. If you notice that physical or mental exertion triggers severe exhaustion that lasts for days, this is a significant warning sign.
Warning Sign #2: Excessive, Persistent Fatigue (Affects 69% of Patients)
What it looks like:
Overwhelming exhaustion that doesn’t improve with sleep or rest
Feeling exhausted upon waking, even after a full night’s sleep
Fatigue that interferes with work, social life, and basic daily activities
Described as “bone-deep” or “crushing” fatigue
How it differs from normal tiredness:
Normal tiredness: Improves with rest; comes and goes; doesn’t prevent basic functioning
PVS fatigue: Constant; severe; doesn’t respond to rest; prevents normal activities
Duration matters: Acute post-vaccine fatigue resolves within days. If your fatigue has lasted 4+ weeks and shows no signs of improving, this could indicate PVS.
Associated symptoms:
Unrefreshing sleep
Need to rest frequently during the day
Can’t maintain previous work schedule
Simple tasks (showering, cooking) become exhausting
Warning Sign #3: Neurological Symptoms (Affects 63% of Patients Each)
PVS frequently causes neurological symptoms across three categories:
Headaches or migraines (often severe and persistent)
Dizziness or vertigo
Ringing in ears (tinnitus)
Why this matters: When neurological symptoms appear shortly after vaccination and persist for weeks or months, especially when combined with other PVS symptoms, this strongly suggests Post-Vaccine Syndrome rather than coincidental neurological issues.
Warning Sign #4: Dysautonomia and Cardiovascular Symptoms
What is dysautonomia? Dysfunction of the autonomic nervous system, which controls involuntary bodily functions like heart rate, blood pressure, and digestion.
Common cardiovascular symptoms in PVS:
Heart palpitations: Feeling your heart racing, pounding, or skipping beats
Tachycardia: Elevated heart rate, especially when standing or with minimal activity
Orthostatic intolerance: Dizziness, lightheadedness, or near-fainting when standing up
Blood pressure irregularities: Sudden drops or spikes
Chest discomfort: Not typical angina, but feeling of pressure or discomfort
How common is this? Research shows that dysautonomia symptoms—particularly orthostatic intolerance and tachycardia—are frequently reported by PVS patients and often overlap with POTS (Postural Orthostatic Tachycardia Syndrome).
Red flags requiring immediate medical attention:
Severe chest pain
Shortness of breath at rest
Heart rate over 120 bpm at rest
Fainting or loss of consciousness
If you experience these emergency symptoms, seek immediate medical care or call 911.
Warning Sign #5: Sleep Disturbances
What it looks like:
Insomnia despite being exhausted
Waking frequently during the night
Unrefreshing sleep (waking up as tired as when you went to bed)
Disrupted sleep patterns or circadian rhythm issues
Difficulty falling asleep or staying asleep
Why sleep problems matter in PVS: Sleep disturbances in Post-Vaccine Syndrome aren’t just “can’t sleep because I’m stressed.” They’re often part of the autonomic nervous system dysfunction that characterizes the condition.
Many PVS patients report that they’re utterly exhausted but cannot sleep well, creating a vicious cycle of fatigue and poor rest.
Warning Sign #6: Multi-System Symptoms
Post-Vaccine Syndrome often affects multiple body systems simultaneously. Here are commonly reported symptoms:
Gastrointestinal Issues:
Nausea
Significant weight loss or gain (without dietary changes)
Loss of appetite or changes in appetite
Digestive problems
Abdominal discomfort
Musculoskeletal Symptoms:
Muscle pain (myalgia) or weakness
Joint pain or stiffness
Muscle twitching or fibrillations
Temperature-sensitive muscle pain (worsens with cold or heat)
Temperature Regulation Problems:
Inability to regulate body temperature
Feeling excessively hot or cold
Low-grade fevers that come and go
Chills or sweating unrelated to activity
Immune System Issues:
Frequent infections or illness
Slow healing
Reactivation of viruses (e.g., Epstein-Barr Virus – found in many PVS patients)
The multi-system nature is a key diagnostic feature. If you’re experiencing symptoms across several different body systems that all started around the time of vaccination, this pattern strongly suggests PVS.
Warning Sign #7: Psychological and Emotional Impact
Important distinction: The psychological symptoms in PVS are a result of the physical illness, not psychosomatic or “all in your head.”
According to the Yale LISTEN Study, in the week before completing their survey, PVS patients reported:
Anxiety: 76% of patients
Depression: 76%
Feelings of helplessness: 80%
Feelings of hopelessness: 72%
Overwhelming worry: 81%
Feeling fearful: 82%
Why these feelings occur:
Actual physiological changes to the body (ie: brain inflammation)
Chronic illness is emotionally devastating
Many doctors dismiss or don’t recognize PVS
Patients often feel gaslit or not believed
Loss of previous quality of life
Uncertainty about recovery
Inability to work or maintain normal activities
This is NOT psychosomatic illness. The psychological symptoms are the natural emotional response to living with a debilitating, poorly recognized chronic condition. Multiple studies have identified biological markers (elevated interleukins, receptor antibody changes, persistent spike protein) that confirm PVS is a somatic (physical) condition.
How Post-Vaccine Syndrome Differs from Acute Vaccine Side Effects
It’s crucial to distinguish between acute vaccine reactions and Post-Vaccine Syndrome.
Significant impairment of daily functioning; many unable to work
Resolution
Does not resolve on its own; requires specialized treatment
The key difference: Post-Vaccine Syndrome symptoms don’t improve over time without treatment. Some acute vaccine side effects resolve completely within days.
How Post-Vaccine Syndrome Differs from Long COVID
Many people—including doctors—confuse Post-Vaccine Syndrome with Long COVID because the symptoms are remarkably similar. We also believe this is why study after study says Post-Vaccine Syndrome is “rare”. However, there are key differences.
Long COVID: History of positive COVID test or confirmed infection
PVS: Negative COVID tests; no evidence of prior infection
Timing:
Long COVID: Symptoms begin during or after COVID infection
PVS: Symptoms begin vaccination
Spike Protein Source:
Long COVID: Spike protein from actual SARS-CoV-2 virus
PVS: Spike protein from vaccine (mRNA-induced production)
Important Overlap:
Both conditions involve:
Persistent spike protein in the body
Multi-system symptoms
Exercise intolerance and post-exertional malaise
Dysautonomia
Cognitive issues
Similar treatment approaches
What if I had COVID AND got vaccinated?
Some patients have overlapping exposures, which can complicate diagnosis, but not treatment. In these cases, a detailed timeline looks at:
When did COVID infection occur?
When did vaccination occur?
When did symptoms start or significantly worsen?
Many patients report being relatively recovered from COVID but developing severe symptoms after vaccination, suggesting the vaccine triggered or exacerbated the condition.
In fact, research shows that many PVS patients meet diagnostic criteria for one or more of these conditions.
4. Normal Test Results
Many PVS patients have normal or near-normal results on standard tests:
Normal bloodwork
Normal imaging (MRI, CT scans)
Normal cardiac workup
Normal neurological exams
This leads doctors to conclude “nothing is wrong” when, in reality, the standard tests aren’t measuring the right markers.
Emerging Diagnostic Markers for Post-Vaccine Syndrome
While there’s no single definitive test yet, research has identified several biological markers associated with PVS:
1. Persistent Spike Protein
Yale researchers found that some PVS patients have detectable spike protein in their blood more than 700 days (nearly 2 years) after vaccination.
Normal: Spike protein typically clears within days to weeks after vaccination.
PVS: Persistent spike protein suggests the body is unable to clear it normally, potentially triggering ongoing inflammation and symptoms.
What this study misses, and what our colleagues (such as Vedicinals) are researching, is spike protein persistence intraceullarly or in-tissue (Yale only looked at circulating). We believe strongly that uncovering spike protein prevalence in tissue will create a much stronger signal for both potential PVS and Long Covid
2. Elevated Inflammatory Markers
Studies have found that PVS patients often have:
Elevated Interleukin-6 (IL-6): Found in over 80% of PVS patients
Elevated Interleukin-8 (IL-8): Also found in over 80% of patients
These cytokines indicate ongoing inflammation
3. Altered Receptor Antibodies
Research from Germany identified significant changes in specific receptor antibodies in PVS patients:
Angiotensin II Type 1 Receptor (AT1R) antibodies: Increased in PVS
Alpha-2B Adrenergic Receptor antibodies: Decreased in PVS
Combined with IL-6, these markers can distinguish PVS from normal post-vaccination response with up to 90% accuracy
4. Epstein-Barr Virus (EBV) Reactivation
Yale researchers found that individuals with PVS were more likely to have evidence of reactivated EBV, suggesting the vaccine may have triggered viral reactivation in susceptible individuals.
5. Autoimmune Markers
Some PVS patients show:
Presence of autoantibodies
Immune complexes in tissue biopsies
Other markers of immune system dysfunction
Important caveat: These tests are not yet widely available or standardized for clinical use. They’re primarily being used in research settings. However, they confirm that PVS is a real, measurable, biological condition. It is not psychosomatic.
Specialized clinics like Leading Edge Clinic stay current on the latest diagnostic advances and can order appropriate testing when available.
Self-Assessment: Do You Have Post-Vaccine Syndrome?
Use this checklist to assess whether you may have PVS. This is not a substitute for medical diagnosis, but it can help you determine if you should seek specialized evaluation.
Post-Vaccine Syndrome Self-Assessment Checklist
You may have Post-Vaccine Syndrome if:
☐ Timeline: Your symptoms started days to weeks to months of COVID-19 vaccination
☐ Duration: Your symptoms have lasted 4 weeks or longer (many patients: months to years)
☐ No COVID: You have no evidence of COVID-19 infection (negative tests, no known exposure, no symptoms before vaccination)
☐ Multi-symptom: You have 3 or more of these core symptoms:
Exercise intolerance / Post-exertional malaise
Excessive, persistent fatigue
Brain fog or cognitive issues
Numbness, tingling, or neuropathy
Heart palpitations or dysautonomia
Sleep disturbances
Multi-system symptoms (GI, muscle pain, temperature regulation)
☐ Severity: Your symptoms significantly impact your daily life, work, or ability to function
☐ No other explanation: Your doctor has ruled out other medical conditions, or you haven’t found another diagnosis that explains all your symptoms
☐ Normal tests: You’ve had normal or near-normal results on standard medical tests, but you still feel very sick
☐ No improvement: Your symptoms haven’t improved over time or with standard treatments
What Your Results Mean:
If you checked 5 or more boxes: You should strongly consider evaluation by a physician who specializes in Post-Vaccine Syndrome. Your symptom pattern and timeline are consistent with PVS.
If you checked 3-4 boxes: You may have PVS or a related condition. A thorough evaluation by a knowledgeable provider would be beneficial.
If you checked 1-2 boxes: Your symptoms may be related to other factors, but if you’re concerned, consult with a healthcare provider.
Important: This self-assessment is for informational purposes only. Only a qualified healthcare provider can diagnose Post-Vaccine Syndrome.
What to Do If You Think You Have Post-Vaccine Syndrome
If you recognize yourself in these symptoms, here are the next steps:
1. Document Your Timeline
Create a detailed record:
Date(s) of COVID vaccination: Which vaccine (Pfizer, Moderna, J&J)? First, second, third dose?
Symptom onset: Exactly when did symptoms start? Hours? Days? Weeks after vaccination?
COVID testing history: Any positive tests? When? Any known exposures?
Symptom progression: How have symptoms changed over time?
Impact on life: How have symptoms affected work, daily activities, quality of life?
Why this matters: The temporal relationship between vaccination and symptom onset is crucial for diagnosis. A clear timeline helps your doctor understand your case.
2. Track Your Symptoms
Keep a symptom diary:
Daily symptom severity (scale of 1-10)
Activities that trigger or worsen symptoms
Patterns (better or worse at certain times of day?)
What helps or doesn’t help
3. Gather Medical Records
Collect:
Previous test results (bloodwork, imaging, cardiac tests)
Previous diagnoses or differential diagnoses
Medications tried and results
Other medical conditions or history
4. Find a Knowledgeable Provider
This is the most important step. Not all doctors are familiar with Post-Vaccine Syndrome. You need a provider who:
Recognizes PVS as a real condition
Has experience treating spike protein-related illness
Uses an integrative, root-cause approach
Stays current on the latest research
Won’t dismiss your symptoms
Leading Edge Clinic specializes in Post-Vaccine Syndrome diagnosis and treatment. Our team has treated over 3,500 patients with spike protein-related conditions and stays at the forefront of PVS research and treatment protocols.
We offer:
Comprehensive evaluation and diagnosis
Evidence-based treatment protocols
Nationwide telehealth access (all 50 states)
Compassionate care from providers who understand PVS
While every patient is different, effective PVS treatment typically includes:
Spike Protein Clearance:
Intermittent fasting (promotes autophagy)
Specific supplements and medications shown to help clear spike protein
Protocols to support the body’s natural detoxification and redox
Immune System Support:
Immune-modulating agents to calm overactive immune response
Anti-inflammatory protocols
Treatment of viral reactivation (if present)
Symptom Management:
Medications for dysautonomia, POTS-like symptoms
Pain management protocols
Sleep support
Cognitive function support
Root Cause Approach:
Addressing mitochondrial dysfunction and cell danger response
Mast cell stabilization (if MCAS is present)
Gut health restoration
Micronutrient optimization
Endothelial healing
Important: Treatment is individualized based on your specific symptoms, severity, and response. What works for one patient may need adjustment for another.
Our providers have refined treatment protocols based on thousands of patient encounters and stay current on the latest research. LINK: Meet our providers who specialize in Post-Vaccine Syndrome
The Most Important Thing to Know
If you’re reading this and recognizing yourself in these symptoms, here’s what you need to know:
1. You’re Not Alone
Even with data most likely undercounting Post-Vaccine Syndrome (affecting an estimated 0.02-2% of vaccinated individuals), that still represents potentially 500,000 to 5.4 million people in the United States alone. You are not the only one experiencing this.
2. It’s Real
Despite what some doctors may say, Post-Vaccine Syndrome is:
Recognized by researchers at Yale, NIH, and leading medical centers worldwide
Backed by peer-reviewed published research
Characterized by measurable biological markers
A somatic (physical) condition, not psychosomatic
You are not imagining this. You are not anxious or depressed (or if you are, it’s because of the physical illness, not the cause). Your symptoms are real.
3. You’re Not Being Hysterical
Acknowledging that you’ve been injured by a vaccine doesn’t make you crazy. It makes you honest about your experience.
You deserve medical care regardless of the political implications of your diagnosis.
4. Treatment Is Available
Post-Vaccine Syndrome is treatable. While recovery takes time, and there’s no “quick fix,” many patients see significant improvement with:
Proper diagnosis and recognition of the condition
Evidence-based treatment protocols targeting spike protein clearance and immune modulation
Comprehensive symptom management
Supportive care from knowledgeable providers
5. Early Recognition Leads to Better Outcomes
The sooner you receive proper diagnosis and treatment, the better your chances of recovery. Don’t wait months or years suffering while doctors tell you “nothing is wrong” or that you need antidepressants.
If you recognize the warning signs, seek specialized care now.
6. You Deserve to Be Believed
Too many PVS patients have been dismissed, gaslit, or told their symptoms are psychosomatic. You deserve a doctor who:
Listens to you
Believes your symptoms are real
Takes your suffering seriously
Works with you to find solutions
At Leading Edge Clinic, we see you, we believe you, and we’re here to help.
Take the Next Step
If you’ve recognized yourself in these seven warning signs, don’t wait. Post-Vaccine Syndrome doesn’t improve on its own. It requires specialized diagnosis and treatment.
What you can do right now:
Download our symptom tracker to start documenting your symptoms (COMING SOON)
Q: How long do Post-Vaccine Syndrome symptoms last?
A: Without treatment, symptoms can persist for months or years, and increase in severity. The median duration in the Yale LISTEN Study was nearly 20 months, and many patients had symptoms lasting even longer. With proper treatment, many patients see improvement, though recovery timelines vary.
Q: Can Post-Vaccine Syndrome be cured?
A: While “cure” isn’t the right word for a complex multi-system condition, many patients experience significant recovery with proper treatment. The goal is to reduce spike protein burden, modulate the immune system, and support the body’s natural healing. Many patients return to normal or near-normal functioning.
Q: Will I need to see a doctor in person?
A: No! Leading Edge Clinic offers comprehensive telehealth services to patients in all 50 states. All consultations and follow-ups can be done virtually via secure video appointments.
Q: Does insurance cover Post-Vaccine Syndrome treatment?
A: We do not participate in insurance. Some patients submit their appointment costs to their insurance providers after the fact to try and get reimubrsement. Coverage varies by insurance plan. We recommend checking with your insurance provider. Many of our patients use HSA/FSA funds for treatment costs. We partner with Opus Health for this
Q: What if I’ve already seen multiple doctors who say nothing is wrong?
A: This is extremely common with PVS patients. Standard medical tests often come back normal or show only minor abnormalities, leading many doctors to conclude you’re fine when you clearly aren’t. Specialized providers who understand PVS know how to recognize the condition even when standard tests are normal and know what testing to order to identify biomarkers and guide treatment.
Q: Can I have both Long COVID and Post-Vaccine Syndrome?
A: Yes, it’s possible to have overlapping conditions, especially if you had COVID and then were vaccinated while still experiencing symptoms. A detailed timeline helps clarify the primary driver of your symptoms. But, more importantly, treatment will be extremely similar, if not identical.
About Leading Edge Clinic
Leading Edge Clinic specializes in complex, multi-system illnesses including Post-Vaccine Syndrome, Long COVID, MCAS, and other spike protein-related conditions. Founded by Dr. Pierre Kory and Scott Marsland, FNP-C, we’ve treated over 3,500 patients nationwide using evidence-based protocols and a compassionate, patient-centered approach.
Our team includes physicians and nurse practitioners who are experts in:
Post-Vaccine Syndrome diagnosis and treatment
Spike protein pathology and clearance protocols
Long COVID and post-viral illness
MCAS and immune dysregulation
Complex chronic conditions
Adjunctive Cancer Care with repurposed drugs
We offer telehealth appointments to patients in all 50 states, making specialized care accessible no matter where you live.
Disclaimer: This article is for informational purposes only and is not intended to diagnose, treat, cure, or prevent any disease. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Published: March 2026 Author: Leading Edge Clinic Medical Team
If you found this guide helpful, please share it with others who may be experiencing Post-Vaccine Syndrome symptoms. Early recognition and treatment can make a significant difference in recovery.
If you’re experiencing persistent fatigue, brain fog, heart palpitations, or exercise intolerance months after either COVID-19 infection or COVID-19 vaccination, you’re not alone — and you’re probably confused about what’s actually happening in your body.
At Leading Edge Clinic, we’ve treated over 3,500 patients with spike protein-related illness. The single most common question we hear is: “Is this Long Covid, or is this from the vaccine?”
The answer matters — not because the treatments are dramatically different (they’re not), but because understanding what’s driving your symptoms helps you find the right care and validates your experience when so many providers are dismissive.
Here’s what you need to know.
The Core Similarity: Both Are Spike Protein Illnesses
Before we talk about differences, let’s establish the most important thing: Long Covid and Post-Vaccine Syndrome share the same underlying pathology.
Both conditions are driven by the SARS-CoV-2 spike protein — the component of the virus responsible for binding to human cells and triggering immune response. In Long Covid, the spike protein comes from the virus itself. In Post-Vaccine Syndrome, it comes from the mRNA or adenovirus vaccines designed to teach your immune system to recognize that same spike protein.
The spike protein, regardless of its source, can cause:
Microclotting — tiny blood clots that reduce oxygen delivery to tissues and organs
Mitochondrial dysfunction — reduced cellular energy production, leading to profound fatigue and post-exertional malaise (PEM)
Autonomic nervous system dysfunction — POTS (Postural Orthostatic Tachycardia Syndrome), blood pressure instability, and temperature dysregulation
This is why the symptom overlap between Long Covid and Post-Vaccine Syndrome is so extensive. You’re dealing with the same underlying mechanisms.
Key Differences Between Long Covid and Post-Vaccine Syndrome
While the pathophysiology overlaps, there are meaningful differences in how these conditions develop, how they’re perceived by the medical community, and what patients typically experience.
1. Trigger Event
Long Covid: Symptoms persist for 3+ months following acute SARS-CoV-2 infection. Most Long Covid patients can point to a specific COVID-19 illness — sometimes mild, sometimes severe — that preceded their chronic symptoms.
Post-Vaccine Syndrome (PACVS): Symptoms develop days, weeks, or even months after receiving an mRNA (Pfizer, Moderna) or adenovirus (J&J, AstraZeneca) COVID-19 vaccine. Some patients experience immediate reactions (within hours to days), while others notice a gradual onset of symptoms over weeks.
2. Onset Timing
Long Covid: By definition, Long Covid symptoms last at least 3 months post-infection. Many patients experience a biphasic pattern — they recover from the acute infection, feel better for a period, then crash weeks later with persistent symptoms.
Post-Vaccine Syndrome: Onset can be more variable. Some patients develop symptoms immediately after vaccination (within 24-72 hours). Others experience a delayed onset, with symptoms appearing 2-4 weeks post-vaccination, or even after the second or third dose rather than the first.
3. Prevalence
Long Covid: Estimates vary widely, but research suggests 10-30% of people infected with SARS-CoV-2 develop some form of Long Covid. The condition is now widely recognized (though still poorly understood) by mainstream medicine.
Post-Vaccine Syndrome: Exact prevalence is unknown, many news outlets report Post-Vaccine Syndrome appears to be less common than Long Covid. However, underreporting is a significant issue — many patients who develop symptoms post-vaccination are told their symptoms are unrelated, or due to Covid Infection, which discourages official reporting and makes true prevalence difficult to estimate.
4. Medical Recognition and Acceptance
Long Covid: Mainstream medicine now acknowledges Long Covid as a real condition. The NIH has funded Long Covid research, the CDC tracks it, and most physicians — even if they don’t know how to treat it — at least believe it exists.
Post-Vaccine Syndrome: This is where the experiences of Long Covid and Post-Vaccine Syndrome patients diverge most sharply. Post-Vaccine Syndrome is frequently dismissed by conventional medicine. Patients are often told:
“The vaccine is safe and effective — your symptoms can’t be related.”
“It’s anxiety.”
“It’s a coincidence.”
“Your labs are normal, so nothing is wrong.”
For the first time, mainstream medicine has begun to acknowledge Post-Vaccine Syndrome. A 2024 Yale study formally recognized what our patients have known for years: vaccine-associated Long Covid-like illness is real, measurable, and distinct from Long Covid caused by infection.
But clinical recognition still lags far behind the research. Most Post-Vaccine Syndrome patients spend months or years seeking validation before finding a provider who takes them seriously.
5. Symptom Presentation
The symptoms themselves are remarkably similar, but there are some patterns we’ve observed across thousands of patients:
Long Covid patients more commonly report:
Loss of taste or smell (especially early in the pandemic)
Respiratory symptoms (shortness of breath, chronic cough)
Gradual, progressive worsening over months
Post-Vaccine Syndrome patients more commonly report:
Sudden, acute onset of symptoms (within days of vaccination)
Severe neurological symptoms (neuropathy, tremors, cognitive impairment)
Menstrual irregularities (particularly after mRNA vaccines)
These are tendencies, not rules. We’ve seen every presentation in both patient populations. The symptom overlap is far more significant than the differences.
Symptom Comparison: Long Covid vs Post-Vaccine Syndrome
The table below shows which symptoms are common to both conditions, and which tend to be more prominent in one versus the other. Remember: these are patterns we’ve observed across thousands of patients, not absolute rules. Every patient is unique.
Can be physiological (histamine, inflammation) not just psychological
Headaches / Migraines
✓
✓
High
Often treatment-resistant
Neuropathy / Nerve Pain
✓
✓✓
High
Tingling, burning, numbness; more acute in PACVS
Tremors
✓
✓✓
Moderate
More commonly reported in PACVS patients
Chest Pain
✓
✓✓
High
May indicate pericarditis or myocarditis (more common post-vaccine)
GI Issues
✓
✓
High
Nausea, diarrhea, constipation, GERD
Tinnitus (Ringing in Ears)
✓
✓
Moderate
Persistent ringing or buzzing
Loss of Taste/Smell
✓✓
✓
Moderate
Much more common in Long Covid, especially early pandemic
Skin Rashes / Hives
✓
✓
Moderate
Often MCAS-related
Temperature Dysregulation
✓
✓
High
Inability to regulate body temperature, chills, sweats
Menstrual Irregularities
✓
✓✓
High
Heavy periods, irregular cycles; more pronounced post-mRNA vaccines
Hair Loss
✓
✓
Moderate
Telogen effluvium pattern
Joint Pain
✓
✓
High
Migratory or persistent arthralgia
Muscle Pain
✓
✓
High
Myalgia, often widespread
Vision Changes
✓
✓
Moderate
Blurred vision, light sensitivity, floaters
Key: ✓ = Symptom present ✓✓ = Symptom more prominent in this condition Overlap: Very High (>80% of both populations), High (60-80%), Moderate (40-60%)
What This Table Shows
The overwhelming similarity in symptom presentation is what makes distinguishing Long Covid from Post-Vaccine Syndrome so difficult — and why your timeline and trigger event (infection vs. vaccination) are often the only reliable differentiators.
If you’re experiencing multiple symptoms from this table and conventional medicine has told you “nothing is wrong” because your labs are normal, you’re not imagining it. These are real, measurable manifestations of spike protein pathology — and they require specialized treatment.
Why the Overlap Exists: Spike Protein Pathology
Whether spike protein enters your body via infection or vaccination, it triggers similar downstream effects:
Microclotting
The spike protein binds to ACE2 receptors on the endothelium (blood vessel lining), causing inflammation and microclot formation. These tiny clots reduce blood flow to tissues, leading to:
Brain fog (reduced oxygen to brain)
Exercise intolerance (reduced oxygen to muscles)
Shortness of breath (impaired gas exchange in lungs)
Mast Cell Activation
Spike protein triggers mast cells to degranulate, releasing histamine and other inflammatory mediators. This causes:
Flushing
Heart palpitations
Digestive issues
Skin reactions
Anxiety and hypervigilance (histamine affects the brain)
Immune Dysregulation
The immune system becomes overactive in some areas (autoimmunity, persistent inflammation) and underactive in others (viral reactivation of Epstein-Barr, HHV-6, etc.). The lack of balance in the immune system can be referred to as “dysregulation”, rather than only referring to it as oceractivation or underactivation. The end result is typically immune exhaustion, and can manifest as lower CD4 T-Cell counts).
Mitochondrial Dysfunction
Spike protein damages mitochondria — the energy-producing organelles in your cells — leading to:
Severe fatigue
Post-exertional malaise (PEM)
Exercise intolerance
Cognitive dysfunction
This shared pathology is why treatment approaches for Long Covid and Post-Vaccine Syndrome are fundamentally the same.
Treatment Implications: Why the Distinction Matters (and Doesn’t)
Why It Doesn’t Matter Much for Treatment
The good news: if you have spike protein illness, the treatment approach is similar regardless of the source.
Both conditions respond to protocols that address:
Spike protein clearance
Microclotting reduction
MCAS stabilization
Inflammatory response reduction
Clearance of senescent cells
Cell Danger Response modulation
Immune modulation
Mitochondrial support
Viral reactivation management
Foundational health approaches
At Leading Edge Clinic, we use the same foundational approaches for both Long Covid and Post-Vaccine Syndrome patients. The personalization comes from your specific symptom presentation, not from which spike protein source triggered your illness.
Why It Does Matter
Even though treatment is similar, the distinction matters for three reasons:
1. Finding a Provider Who Believes You
Long Covid patients can usually find a provider willing to acknowledge their condition. Post-Vaccine Syndrome patients face significantly more dismissal. Knowing what you’re dealing with helps you seek care from providers (like us) who specialize in both.
2. Understanding Your Timeline
Post-Vaccine Syndrome patients often experience more acute, sudden onset — which can be frightening. Knowing this is a recognized pattern helps contextualize your experience.
3. Preventing Re-Exposure
Both Long Covid and Post-Vaccine Syndrome patients need to be cautious about reinfection (which can worsen symptoms). We know that continuous spike protein exposure will further trigger related symtpoms, and increase the number of senescent cells. Understanding your trigger helps you make informed decisions about future exposures.
How Leading Edge Clinic Treats Both Conditions
We’ve treated over 3,500 patients with spike protein illness — both Long Covid and Post-Vaccine Syndrome. Here’s how we approach care:
Comprehensive Initial Evaluation
We don’t care whether your spike protein came from infection or vaccination. We care about:
Which body systems are affected (cardiovascular, neurological, immune, etc.)
The severity of your symptoms
Your specific symptom triggers
Any viral reactivations or co-infections
Your prior treatment history and what’s worked (or hasn’t)
You’re not left on your own between appointments. Our Registered Nurses check in every other week to monitor your response, adjust protocols, and escalate concerns to providers immediately if something isn’t working.
Telehealth in All 50 States
We see patients nationwide via secure telehealth. You don’t need to live near us to receive specialized care.
Long Covid and Post-Vaccine Syndrome are not identical conditions, but they share the same underlying pathology: spike protein-driven illness.
The key differences are:
Trigger: Infection vs. vaccination
Onset timing: Gradual vs. often more acute
Medical recognition: Acknowledged vs. frequently dismissed
But the similarities far outweigh the differences:
Both involve spike protein pathology
Both cause microclotting, MCAS, immune dysregulation, chronic Cell Danger Response, senescent cell cycle, mitochondrial dysfunction
Both respond to similar treatment protocols
Both require specialized care from providers who understand spike protein illness
If you’re struggling with persistent symptoms after COVID-19 infection or vaccination, you’re not imagining it. You’re not alone. And there are providers who can help.
Can you have both Long Covid and Post-Vaccine Syndrome?
Yes. Some patients develop Long Covid from an initial infection, then experience worsening symptoms after vaccination. Others develop Post-Vaccine Syndrome first, then experience symptom escalation after a subsequent COVID-19 infection. The spike protein exposures are cumulative, as is the build up of senescent cells
How do I know which one I have?
The timeline is your best clue. If your symptoms started within days to weeks to months of vaccination (and you hadn’t recently had COVID), it’s likely Post-Vaccine Syndrome. If symptoms followed a documented COVID infection and persisted for months, it’s likely Long Covid. If you’ve had multiple exposures (infection + vaccines), you may have elements of both.
Will my doctor test me to determine which one it is?
There’s no single test that definitively distinguishes Long Covid from Post-Vaccine Syndrome. Diagnosis is clinical — based on your history, timeline, and symptom pattern. Some providers order microclot testing, inflammatory markers, or immune panels, but these show similar abnormalities in both conditions.
Does it matter for insurance coverage?
In the U.S., both conditions are generally treated the same by insurance (though coverage for integrative treatments is often limited regardless). The diagnosis code used may vary, but treatment coverage depends more on the specific interventions prescribed than on whether the spike protein came from infection or vaccination.
Are the outcomes different for Long Covid vs. Post-Vaccine Syndrome?
We don’t have enough long-term data to say definitively. Anecdotally, we have seen Post-Vaccine Syndrome patients typically have more severe presentations, with a longer road to recovery. However, this isn’t always the case. The biggest predictor of outcome isn’t the spike protein source — it’s how quickly patients receive appropriate treatment and how severe their initial presentation was.
About the Author: This article was written by the clinical team at Leading Edge Clinic, which has treated over 3,500 patients with Long Covid, Post-Vaccine Syndrome, and related spike protein illnesses. Our providers include Dr. Pierre Kory (MD, MPA), Scott Marsland (FNP-C), India Scott (FNP-C), and other specialists in complex chronic illness.
Medical Disclaimer: This article is for educational purposes only and is not a substitute for personalized medical advice. If you’re experiencing persistent symptoms after COVID-19 infection or vaccination, please consult with a healthcare provider experienced in treating spike protein-related illness.