Taking a break from writing Lightning Bug every week since October 2023 has been helpful, in order to rest, ponder and organize ideas in my mind. I like noticing what bubbles up to the top. Today’s post is a nod to one of my favorite Beatles songs, but also a hypothesis that sharing how I have personally implemented a lifetime of learning could be instructive, and even invite thoughts and questions from readers regarding their own experiences and strategies.
From A day in the life by The Beatles
Woke up, fell out of bed
Dragged a comb across my head
Found my way downstairs and drank a cup
And looking up, I noticed I was late
Found my coat and grabbed my hat
Made the bus in seconds flat
Found my way upstairs and had a smoke
And somebody spoke and I went into a dream
MORNING
When the alarm goes off at 6:10am, I snuggle up to my beloved for some spoony physical closeness. Our orange and white cat, Renny, who will have spent the night on one of our pillows, settles back onto our heads. After two snoozes, Renny gets up, we role away from each other, I turn on my left side, kick out my right leg, and push myself up to a sitting position. I take the Arc Microtech device I wore during the night off my ankle and set it aside to recharge. I then use my fingertips to perform a percussive self-massage up, down and across my chest. This was a lesson from Jovanna, née Joan Perna, the mother of my friend Larami.
Jovanna was a hot-blooded Sicilian, masseuse, nudist, and pursuer of many things alternative. Never mind that I was a little squirmy touching and being touched by this beautiful woman, twice my age. It was a hot July summer morning and she was visiting us in the third-floor walkup apartment we were sharing in Philadelphia’s Center City. Jovanna explained that this massage technique helps brings blood flow to the lungs and thus the brain and rest of the body, which eases and speeds one’s waking. Lesson learned, I never stopped, and have done it every morning for the last thirty six years.
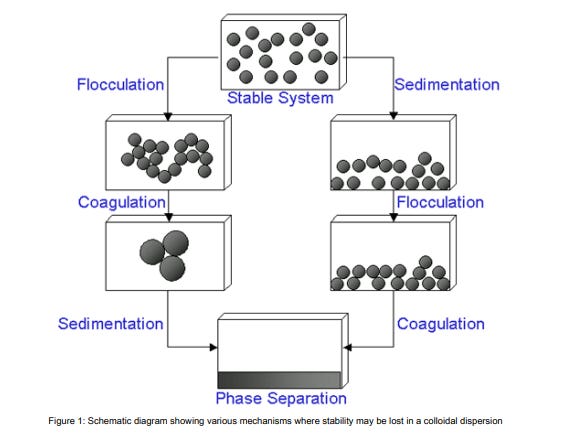
As we make the bed, I straighten out the cord to the grounding pillow cover underneath my pillow case, and straighten out the grounding sheet on top of the fitted sheet at the foot of the bed. Grounding, which can also be accomplished by walking on the earth in our bare feet, or touching soil and plants with our bare hands, is a manner of accepting negative electrons freely donated by the earth. This negative energy helps move the charge of our cells back towards negative polarity, which the Substack writer A Midwestern Doctor discusses as the Zeta Potential. Spike protein, lipid nanoparticles and other pathogens disrupt the Zeta Potential, and adversely impact the permeability of our cells. EMF also adversely the Zeta Potential, and grounding sheets are a simple way to push back, which helps weaken the energetic attraction of platelets and red blood cells (RBCs) to each other in aggregates, thus reversing flocculation.
“In certain circumstances, the particles in a dispersion may adhere to one another and form aggregates of successively increasing size, which may settle out under the influence of gravity. An initially formed aggregate is called a floc and the process of its formation flocculation. The floc may or may not sediment or phase separate. If the aggregate changes to a much denser form, it is said to undergo coagulation. An aggregate usually separates out either by sedimentation (if it is more dense than the medium) or by creaming (if it less dense than the medium). The terms flocculation and coagulation have often been used interchangeably. Usually coagulation is irreversible whereas flocculation can be reversed by the process of deflocculation.” https://www.research.colostate.edu/wp-content/uploads/2018/11/ZetaPotential-Introduction-in-30min-Malvern.pdf
Within minutes of rising from bed, ten at the most, I drink a thirty-two ounce glass of roomish-temperature distilled water, and then pour another, to drink within the next half hour. Mohit Bali taught me about water upon waking. Mohit, a reclusive computer geek from Eastern India, was a quad-mate my freshman year at Susquehanna University. One day he completely surprised me—and slightly creeped me out—by offering this observation. “Scott, I think that you need to drink more water. You should do this every morning when you first arise. Every human being wakes dehydrated, because our body has been repairing itself during the night, which uses fuel and makes waste. This is an ancient teaching of Ayurvedic medicine. Here is a mason jar. Fill this and drink a glassful of water every day upon rising.” Mind you that he rarely came out of the dark lair of his room, let alone conversed. Then he disappeared back into his room, leaving me standing there with the mason jar in my hand. Weird. Crazy weird. But, I took his advice and still do to this day.
Why distilled water? I’m betting that this is where the first alternative perspectives, questions and strenuous objections will arrive, such as, we should add trace minerals or a pinch of Celtic sea salt to our water. Well, there was this older African American man. He had a riotous head of grey hair, and he smelled like basement and oil furnace. I would encounter him sometimes in the grocery story where I worked while attending nursing school in Philadelphia about thirty years ago. I’m not sure why or how we hit it off, but we both lived within walking distance of the store, and on more than a few occasions he would stop by our little Trinity house and we’d sit on the steps and visit. One day he brought me a book called Water Is Life, which laid out the argument that the inorganic minerals and elements, including limestone, which were dissolved in water, accumulated over time in our bodies and led to the development of atherosclerotic plaques and decreased kidney function. He was preaching, and this was his sermon to me. It made enough sense and Philly tap water tasted terrible. We were spending money from our limited budget on spring water, so we pivoted and purchased a water distiller from Waterwise in Florida. With occasional postal trips to Florida for maintenance, that first distiller lasted more than twenty years. We are now on our fourth generation….
Each morning with that first glass of water, I take one capsule of NAC Augmentata from Italy, which breaks the disulfide bond between spike and ACE-2 receptors, along with 500mg of esterified (Ester) Vitamin C. There is synergy between NAC and Vitamin C such that together, they have more antioxidant and immune-supporting action than either by itself. Each acts through different mechanisms. Vitamin C can directly scavenge free radicals, while NAC boosts the level of glutathione, another powerful antioxidant. Vitamin C can also help regenerate oxidize glutathione back to its reduced form, thus maintaining higher levels of active glutathione in the body. NAC Augmentata is made by ZeroSpike in Italy, a small non-profit start up which is trying to save humanity, and at at dose of 200mg is exponentially more effective than other forms of NAC. We source it from our trusted colleagues at Vitahealth Apothecary in NYC, which has been the primary U.S. distributor, although there may be a few new U.S. suppliers at this point.
My introduction to esterified Vitamin C was very personal. I met Chef Robert Lehmann (pronounced LAY-man) at The Commissary Restaurant in Philadelphia, where I was a busboy in the summer of 1989. He later become the Executive Chef of MANNA, a meals-delivery service organization for homebound people with AIDS in Philadelphia. As such he developed diet and nutrition standards for people who are HIV positive. He wrote a book: “Cooking for Life: A Guide to Nutrition and Food Safety for the HIV-positive Community.” When I next returned to Philadelphia during Winter break 1989-1990, I would volunteer with MANNA, where Rob would supervise food preparation and occasionally I delivered those meals to the beautiful gay men who were languishing during what some call Fauci 101. Rob taught me that esterified Vitamin C could deliver much needed nutrition and immune support to these fragile people without upsetting or harming their stomachs. I took note.
While in the kitchen finishing my second glass of water, I light the burner under the old English-made copper teapot, and when it whistles, I fill up my thermos and leave the lid off to let it cool a bit before making green tea with loose leaves. As the tea steeps, I stir two tablespoons of Baobab powder into a cup of water, and divide this into two other thermoses, which I then fill with water; one for my wife and one for me. Both the green tea and the Baobab have EGCG, which blocks spike entry into cells. The Baobab has many other benefits, but serves to promote a robust and diverse microbiome in the gut. I bring the green tea, Baobab and half gallon of distilled water to my office, and drink these three beverages over the course of the day.
Meanwhile my wife has made her way to the back, lifting shades, opening curtains, and turning the Wi-Fi back on as we start the day. Some time ago we made it a habit to turn the Wi-Fi and all of our electronic devices off at bedtime. This routine was inspired by Dr Robert O Becker, a Veterans Administration researcher and orthopedic surgeon who studied how energy can be used to heal—and whose research provided the scientific basis of the Arc Microtech device we use with more than three hundred patients. Given his (now quaint) concerns in the 1980s re: CB radios and FM radio towers, it is a short skip and a jump to realize that nothing good will come of the barrage of EMF we live in on a daily basis. The very least we can do it dial it back when we are trying to sleep.
I then head for the sauna with Malcom, the big black cat with soulful eyes who we adopted in January. He likes to join me in the Sauna Space near infrared (NIR) sauna for some chin rubs and warmth. I get naked as the day I was born, sit on the towel-draped stool, and over ten minutes, do two 360 degree rotations of exposure to the lights. Ten minutes is the sweet spot to help repair mitochondrial function and increase ATP production; not five, and not fifteen, but ten. Thanks for the tip on timing Dr Been!
While I’m in the sauna, I will often pray, or chant. As Quakers say, I hold others in the light. This is when I will seek sustenance, clarity and direction in my care of our complex and chronically ill patients at The Leading Edge Clinic during the upcoming day. When I say “or chant”, I refer to what I learned from our Japanese neighbors Hiro and Akiko Uhuru when we lived in Philadelphia. I remember them taking me to a gathering and chanting session of their Buddhist organization, and really not knowing what to think about it. After we left Philadelphia, they sent me a book which gave me some insight. Namu Myōhō Renge Kyō (南無妙法蓮華経) are Japanese words chanted within all forms of Nichiren Buddhism. In English, they mean “Devotion to the Mystic Law of the Lotus Sutra” or “Glory to the Dharma of the Lotus Sutra”. It is a vow, an expression of determination, to embrace and manifest our Buddha nature. It is a pledge to oneself to never yield to difficulties and to rise above one’s suffering. At the same time, it is a vow to help others reveal this law in their own lives and achieve happiness. I can get behind this. For those of you who have seen The Life of Pi (one of my top ten favorite movies ever), you may appreciate the main character’s curiosity, embrace and practice of multiple spiritual practices in his joyful life. It is one thing to pray, but quite another to chant Namu Myōhō Renge Kyō the hour and a half home from a twelve hour COVID shift in the Emergency Department (ED).
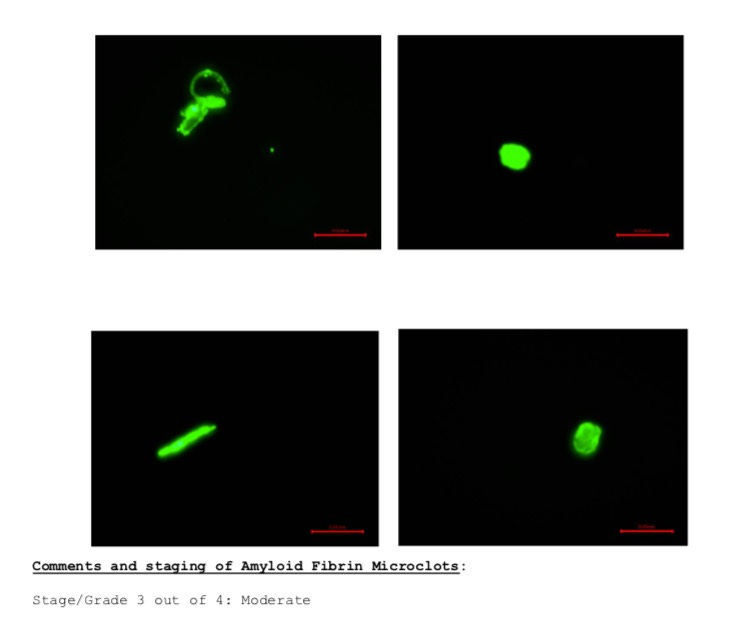
Our time in the sauna complete, Malcom and I step out, and I drink my second glass of distilled water. This glass of water is accompanied by 4,000FU of Nattokinase and two capsules of Flavay. Both are used to help breakdown the amyloid fibrin micro clots which we all have secondary to the spike protein in our bodies. Flavay is small molecule pycnogenol, using a patented formula which not only decreases platelet aggregation to other platelets and the walls of our blood vessels, but also has an antihistamine effect within the blood vessels.
Next stop is the bathroom where our little Manx cat, Sophie, is waiting for me on her cat mattress, taking second shift following my wife’s shower. Near the end of the shower, I take a deep breath and as I’m blowing it out, turn off the hot water. For sixty slow, deep breaths, I turn as the cold water falls on my body. More than a year ago, I developed reservations about using cold water exposure in post-acute sequelae of COVID (PASC) and vaccine injury, as I understood how prevalent micro clotting was, and constriction of blood vessels in cold water was concerning. My personal experience was that an old surgical site in my groin would start to ache in the cold water, and the numbness/tingling in my toes and feet would worsen. Since February of this year however, my appreciation and treatment of mast cell activation syndrome (MCAS) in my patients has grown by the day. Knowing that cold exposure can be helpful in dampening MCAS, I’ve revisited this intervention. It’s worth noting that summer is the ideal time to initiate this practice, as it gives us time to build up brown fat cells so that when the weather turns cooler, we will better be able to tolerate the cold.
Brown fat cells, cold exposure, and the Wim Hof Method were introduced to me by my cousin Danny more than five years ago during a Marsland family vacation at the Jersey shore. These days, Danny is working as a welder and helping to build a nuclear aircraft carrier for the US Navy…so, not a medical professional. But, I’ll say that he has been years ahead of the curve on a number of health-related topics. He was the first person to ask me about IVM at the beginning of the pandemic, back when I thought vaccines were a good thing and that I could trust my ED pharmacist colleagues. Boy was I wrong! Brown fat cells came up in two continuing education lectures I watched pre-pandemic, when the topic was medical and about scientific developments around managing obesity. Yes, I was thinking, “Damn, Danny was right about this too!” We were all born with brown fat cells, and quickly lost them, because we are modern creatures of comfort, with central heating and air conditioning in our homes, our cars, and workplaces. Brown fat cells, unlike the white fat cells that adorn our bellies and buttocks, burn energy and can produce heat. This is how/why earlier humans could withstand the elements with greater tolerance than us pampered modern folks.
After my shower, I apply a roll-on deodorant which is made by the German company Weleda. It is essential that no one use a deodorant which has aluminum in it. The aluminum will be absorbed through our pores, and into our lymph glands as well as, ultimately, our blood stream. The aluminum will promote flocculation (mentioned above), a nasty aggregation of platelets, red blood cells and fibrin, which will make a sludge in our blood stream and further impair our circulation.
I get dressed and head into the kitchen where I unplug my Arc Microtech from the charger and put it back on my ankle for it’s first cycle of the day. This device was introduced to us by our British colleague Dr Tina Peers, who at that time had seen tremendous benefit in more than 140 people. This included her father, who went into heart failure after COVID shots, and whose cardiac pumping function recovered from 40 to 55% with use of the device. The Arc is a genetic repair tool. It systemically decreases inflammation, repairs mitochondrial damage so that ATP production returns, and influences genetic expression to limit pathology and encourage cellular repair.
Sophie and Renny are both standing by, hoping for a lick of butter from my fingertips as I prepare my breakfast. For many years I would make toast with Hazelnut butter, nutritional yeast, and then prepare oatmeal with flax seeds, prunes, dates, apple and Silk soy milk. Recently I have shifted to a lower carb routine, with free-range eggs, sausages with local pasture raised pork, and a single slice of Vollkornbrot rye bread with butter and nutritional yeast.
Renny volunteers to clean up the egg yolk from my plate when I’m done. If it isn’t too hot, he’ll settle in for a post-prandial nap by my side while I read a few pages of a study or clinical book while I’m eating. Morning is probably the best time for our brain to take in new and complex information such as this. I try not to turn my phone back on until this time, allowing at least two hours of electronics-free time from when we first woke. Our nervous systems need regular pauses and vacations—fasts if you will—from our electronic devices.
After washing the dishes, I take 4.5mg of LDN liquid, and 1.5mg of Ketotifen. Then I wash down three fistfuls of pills with water containing 25mg of Lugol’s 5% iodine, and 50 drops of Boiron Ribes Nigre gemmotherapy. The pills include Eliquis 2.5mg, Plavix ¼ tab, Aspirin 81mg, IVM 18.5mg, Bacopa 500mg, Lithium 5mg, Dr Wilson’s Adrenal Stress and Adrenal Rebuilder, a B-complex, Resveragen, Ester-C 500mg, pre-natal DHA/EPA, Antronex, and Bromelain 500mg.
I head to the bathroom and brush my teeth. A recent arrival in our routine is a water flosser. Where has this been my whole adult life? It would have saved us a lot of money in dental bills for sure. When it comes to dentist visits, I’m like a little boy, wanting to get the gold star because my gums don’t bleed when probed, and I hear that I’m one of “the best” patients. Dr Richard Oberly is my dentist, and has become a friend over the last twenty four years. He was the second person, after my cousin Danny, who asked me about IVM. I give him a gold star for persisting in teaching me, as an adult, over a period of years, how to correctly brush and floss my teeth. Gold stars aside, good oral hygiene is key to optimal health, as chronic inflammation of the gums and its causes have been associated with heart disease, diabetes, and dementia. We simply must take the time to gently and thoroughly clean our teeth, gums, and mouth before we carry on with our day.
Moving to the kitchen, I put on my backpack and call out to my wife that I’m leaving. I move into the mud room, where our youthful and bright black cat Charlotte is swishing her tail as she watches the morning attendees at the bird bath, including birds, groundhogs, red squirrels, grey squirrels and chipmunks. Kerrie and I hug, there are kisses to lips, left cheek, right cheek, lips, and wishes to each other for a good day. And up the hill I go….
P.S. I opted to leave out the nitty-gritty re: the fistfuls of pills I swallow, and will take this up in my follow up piece(s) to A day in the life.