Little grey cells – by Scott Marsland, FNP-C
[ad_1]
PAST
Today I have a facility with numbers and finances, but that wasn’t always the case. When I was a boy, I delivered papers for the New Britain Herald. It was an afternoon paper, back when there were such things. In my substack Capital C Characters, I wrote about the “bionic” man who was one of my customers. I had about 60 customers. Depending on the weather — and how many stops I made for socializing— it took me anywhere from a half hour to an hour to bicycle around delivering their papers after school.
On Saturdays I needed to collect payment. Some customers had subscriptions through the office and mailed in their monthly checks. Most of my customers paid on a weekly basis. I had a little flipbook with tiny, dated coupons that I would tear out and give to the customer when the payment was made. I think this was good practice for life because it meant handling money on a regular basis and, by extension, that means dealing with people’s idiosyncratic quirks around money.
Most customers were home and answered the door on Saturday, knowing I would be there to collect. But there were always a few who either weren’t home or didn’t answer, even though I suspected that they were in there somewhere. This gave me an early lesson in persistence.
Weather in my area of Connecticut at that time could still deliver extreme conditions. Winters were marked by bitter cold and plenty of snow. Flash rain storms with thunder and lightning, gale force winds, hundred degree days with high humidity, not to mention the ferocious dogs that wanted a piece of me: it was all part of the mix. There was one day that I just didn’t feel up to delivering papers and so I didn’t. I delivered Tuesday’s paper with Wednesday’s paper. There weren’t a lot of complaints, but the ones that I did get stung. This was my introduction to providing good customer service while managing extreme dissatisfaction.
At least three times a year my family would leave town on a road trip. This was usually to spend Thanksgiving and Easter with both sets of grandparents in Pennsylvania, and sometimes a week at the shore with the Marsland clan. My parents weren’t micro-managing my affairs, and so this meant that it was up to me to find a substitute to meet my obligations, and pay him well enough that he found it worth his time and effort. This was the upside of my not having helicopter parents. I had to figure this stuff out on my own as early as fourth grade.
Zhivago Velasco and Larry Lebatique became my go-to guys to cover my route. They were both classmates, first generation Americans of immigrant Filipino families. With a memory that astounds me today I was able to easily recall the street names and house numbers for all of my customers and write a list from which Zhivago and Larry could deliver the papers. If I was lucky and most people paid their weekly bill, I would net about $10 a week, which wasn’t bad for 1976. I think that I paid $15 to Larry and Zhivago. I intuitively understood that they didn’t have the relational capital or emotional investment in this enterprise that I did and accordingly I would have to compensate them with more financial reward.
On the other end of things, I would have to hand over the payments to my handler, the nameless adult who dropped off the bundle of newspapers in our driveway six days a week. Every Sunday evening, I would be sitting at the kitchen table with a pencil and eraser doing long addition, subtraction and multiplication to determine the amount of cash and coins I needed to leave in an envelope taped to the storm door for the handler to collect every Monday morning. I never got it right. I never left enough. I tried and tried and tried to understand the formula. I’m pretty sure that I called the main office more than once to try and get some insight. The experience which I had around paying my handler, probably planted the seed for me to become a union agitator and organizer many years later.
What I knew for sure was how hard I worked. And that it felt like I was being cheated. Even worse was that I couldn’t crack the code and challenge my handler, so that his skimming capitalist enterprise could and would exploit my cheap labor. It’s not like I had a mortgage to pay, but I did depend on that money to buy the model planes I liked to build and the candy of which my mother disapproved. I wanted to buy the sugary Fruit Loops and Applejacks cereals that would never make it into our family shopping cart. I even ventured out into more “exotic” cuisine like yogurt, and the stir fried rice from the local Chinese takeout. I acquired an appreciation of the scent of incense from the New Age store, and bought some Phillies blunt cigars, and Malboro cigarettes. So, I continued to ply my trade, knowing that I was being exploited, but was getting some reward that definitely improved my quality of life.
RECENT PAST

When the nuclear power plant at Fukushima, Japan melted down in March 2011, I felt despair which landed on top of my feelings at following the prolonged war in Iraq. I determined that the most achievable and sensible way to counteract that despair was to put solar panels and solar thermal tubes on the roof of our house. My wife certainly didn’t stand in my way, but she never had— and still doesn’t have— the same enthusiasm which I did, which was necessary to pull it off.
We needed to replace the roof around the same time. My wife had been working in construction for 6 to 7 years at that time, co-owner of a small residential building company. Their preferred roofing material was corrugated metal, and some of their customers from the Ithaca community and its environs would install solar panels on their roofs. This meant drilling holes through the corrugated metal which not infrequently led to leaks—and call backs!
At the time, New York State had generous rebates for solar electric, solar thermal, and reflective roofing material. My wife and I are generally inclined to pay more for something that’s built well and will last longer, and we decided that installing a standing seam roof would be the best investment of our money. The racks for the solar panels and tubes could be attached to the seams without compromising the integrity of the roof. Of course, standing seam metal roofs are only slightly less expensive than slate.
We obtained a home equity loan, borrowed more than $10,000 from our stepmother Betty Ann (who took this out of her retirement in order to bridge the expenses until the NY rebates came in) and signed contracts for a roofer and solar installation.

That was thirteen years ago. Given that the roof hasn’t leaked, gas and electric prices have increased exponentially, and the solar thermal tubes paid for themselves by 2019, I think we made a good choice. My wife might still disagree. Her partner in residential construction was very critical in 2011, quipping that “You’ve got a Cadillac sitting on top of your house.” I’m curious, but only slightly, what he would say today.
What I didn’t know back then, but I know now, is that solar electric panels are no bargain for the global economy and environment. The harm to the environment from mining and processing the raw materials to make them, exploitation of cheap labor, and rebates which ultimately serve bigger corporations that finance installation of PV panels on fertile farmland, taking it out of commission… these are all concerning and give me reason to pause.
But let me tell you, when I see neighbors whose 30 year asphalt shingle roof is being replaced after 10 years, I count myself lucky. It gives me great pleasure every time I come down to the basement on a sunny day and see that the domestic hot water has been preheated to more than 100° by the sun. We resell our excess electricity to our utility company. It’s delightful to see the drop in both the charges for supply and generation of electricity sold to us at retail by NYSEG, now a Spanish conglomerate, but retaining its New York name.
These investments would not still be useful if there were not several passionate men who arrived in our moments of need to help troubleshoot and maintain the electricity, plumbing, and various components of these complex systems from which we benefit.

It is here that I can write about one of the finest human beings I ever had the pleasure of knowing. Bob Nape and I first met in 2005 when we were both helping to start the Ithaca Free Clinic (IFC). He had serious carpentry skills and together we put up partition walls and drywall to build out the internal exam rooms of the IFC. The thing is that he didn’t just bring his skills, he brought his warmth, humor, and love of humanity, which made it a joy to be around him.
Bob was a man of long-standing passions. He became keenly interested in solar hot water back in the 70s in Philadelphia. He was also an enthusiastic and probably very good basketball player. He certainly had the height and the speed for it. He was more faithful in living his Catholicism and doing good in the world than the Pope, as exemplified by his perspective and actions from the moment he woke every day. Years after we met through the IFC, Bob started his company Solar Is Hot, through which he helped legacy solar thermal systems dating back to the 1970s, as well as newer ones such as ours, remain functional. I cannot take a hot shower without giving thanks to Bob.
We connected around our mutual challenges with heart disease and arrhythmias, which in my case kept me out of competitive sports, but in Bob’s case never kept him from his basketball games. During the pandemic, he developed complications following acute COVID, had a stroke, and ended up at SUNY Upstate, my previous employer. His loving partner Elizabeth, who also helped start the IFC, attended to him faithfully during his last days, and was at his bedside when he died January 2nd, 2021. I count Bob as one of the many great losses of the COVID era, who I think could still be alive today, but for the war on Ivermectin and all repurposed drugs. An odd twist to our story is that when I signed up for a post office box for the Leading Edge Clinic, it turned out that the one assigned, #6834, had been Bob’s.
Another person who has helped us over the last twenty years of home ownership is David, whose last name I don’t know, but who is the constant presence behind the service counter of an old-fashioned plumbing supply business in Ithaca. I have literally carried in a four foot section of twisty plumbing that I cut out of it’s place under our utility sink, and he helped me identify and assemble the new pieces I would need to replace it. He would guide me with patience and humor every time. And so, for good reason, I trusted him.
In September of 2021 our solar thermal system had a problem, and I didn’t have Bob. There was a puddle of the glycol fluid, which was supposed to be circulating in the system, but was instead pooling beneath the expansion tank. Because I didn’t have a choice, I started reading and watching videos, ordered a new tank, and went to David for advice on a fitting. He gathered what I needed from the warehouse, out of my sight, while I waited at the counter. I paid him and drove home to begin my project.
Eight hours and a lot of cussing later, I was unsuccessful. I had depressurized, disassembled, reattached and re-pressurized the new expansion tank six times, and each time there was a leak around the fittings. My kind, loving, patient wife, was trying to have a productive day in her stained glass studio on the other side of the basement, and it wasn’t going well, because as the hours went on, the number of f-bombs coming out of my mouth was increasing.
I had one lifeline which I hadn’t used…Paul Czarnecki, who was mentioned in my Capital C Characters substack. Via phone and text, I explained my predicament, but even Paul couldn’t get me out of this jam. And it was then, after eight hours of blood, sweat, tears and a blue streak of foul language, that I finally understood what went wrong. My dear trusted David had sold me this:

But he didn’t tell me, it was a combination of these two pieces:

As a result, there was not teflon tape or paste between the threads of these two fittings, and under pressure, the connection was leaking. By the time I figured this out, I had put so much torque on the original two pieces that there was not chance of getting them apart, and David’s store was closed. Off to Home Depot I went, purchased the two pieces, came home, wrapped Teflon tape around the joints, reattached the joint and tank, repressurized, held my breath, and turned the circulating pump on again. I swear that on the other side of the wall, my wife was holding her breath too! This time—success— there was no leak!!!!

To this day, that damn fitting sits on my home office desk, to remind me that if we persist and approach challenges with an open mind, questioning our assumptions, we just might sometimes come up with a solution. We just need time to let the little grey cells of our brain work on the problem.
PRESENT
With the author’s permission (my own), I’m going to reiterate part of what I wrote in my subtack Hot Mess Express, in which I discussed the use of Lithium as a trace mineral.
What about Lithium Orotate? Dr Michael Nehls, the neuroscientist from Germany, has been talking a blue streak about Vitamin D and Lithium Orotate to protect our brains from the onslaught of spike. Pierre and I had the pleasure of a private meeting with Dr Nehls nearly two months ago, and he helped us understand that Lithium Orotate was a key tool in the fight to reclaim our brains in general, and the hippocampi in particular. If therapeutics such as Vitamin B6 (as P5P 50), or 5-MTHF, or L-Theanine are useful to rebalance specific neurotransmitters, then Lithium Orotate is a general tonic which helps rebalance all neurotransmitters, because it reestablishes neuronal connections, decreases neuro inflammation, and enables the brain to start making new neurons. The particulars for inidividual patients have proven to be nuanced. I generally start with 130mg, but India Scott FNP-C prefers to start with 20mg of Lithium Orotate and work up to 130mg, stopping if clinical benefit is achieved earlier. Dr Nehls strongly recommended 130mg for symptomatic patients, dropping back to 20-30mg for maintenance when stability has been achieived. It’s important to note that 20-30mg of Lithium Orotate equals 1mg of active Lithium and 130mg of Lithium Orotate equals 5mg of active Lithium.
Because most health professionals — and many laypeople — have preconceptions about Lithium as solely the province of psychiatry and bipolar schizophrenia, it’s important to note that we are talking about Lithium as a trace mineral. Would you be concerned about toxicity from a pinch of Celtic sea salt in your water, or 25mg of Vitamin C? No. Neither should you be concerned about trace amounts of Lithium which are many times less than the doses used in psychiatry. You can get 1mg of active Lithium by drinking a pricey bottle of San Pelligrino mineral water, or eating a lot of seafood, but you’ll also quickly empty your wallet, and in the case of seafood, there are so many toxins in the ocean that you’ll poison yourself with mercury before you reach therapeutic levels of lithium. And it’s cheap, cheap, cheap. Horbaach makes a 130mg capsule of Lithium Orotate which costs $15 a bottle, including shipping, and provides six months worth of the supplement.
The Leading Edge Clinic has several dozen patients in Canada, and together we find ways to get lifesaving supplements and prescription medication to them, in spite of the totalitarian and life-threatening restrictions which the Canadian government continues to impose upon its citizens. Thanks to one of these patients, this week I came to understand that I was somewhat befuddled about the dosing and active Lithium content of the supplements I was recommending. It is my hope to bring light to this topic, as there is ample potential for confusion.
The form of Lithium which Dr Nehls recommends is Lithium Orotate, and that is primarily because of its bioavailabilty and affordability. The trouble begins with how the different supplement manufacturers label their products, and then how the supplement vendors (we use FullScript for a 30% discount for our patients) catalogue the supplements. From my perspective, Horbaach does the best job in their labeling, as the front of the label states “Lithium Orotate 130mg”, and the back states “Lithium 5mg (from Lithium Orotate).” What follows below is correspondence from three other suppliers of essential Lithium as Lithium Orotate: Vital Nutrients, Pure Encapsulations, and Doublewood. First, Vital Nutrients:
Vital Nutrients – Support
From:support@vitalnutrients.co
To:X
Mon, May 13 at 4:42 p.m.Good afternoon,
Thank you for contacting Vital Nutrients.
There is 500mg of total lithium orotate and 4% is elemental. So 20mg of elemental lithium and 480mg of orithic acid. (for round number purposes)
This is the highest we do carry. We are unable to do a comparison as other companies may source raw materials from other vendors. It would not be an accurate comparison.
If there is anything else we can do today, please let us know.
Omar
Customer Care Representative II
888.328.9992 | vitalnutrients.coOn Mon, May 13, 2024, at 08:41 PM, X> wrote:
To follow up on my previous question…I think the confusion has arisen from the fact that it doesn’t say Lithium Orotate on the front of your bottle, just Lithium. So I read it as 20mg of pure lithium. If it’s not correct, and 20mg is the amount of lithium orotate, then what is the actual amount of pure/elemental lithium in your supplement? If the opposite is true and 20 mg is the amount of pure lithium, what is the amount of lithium orotate per capsule?On Mon, May 13, 2024, at 08:29 PM, X> wrote:
Hello, could you please confirm the amount of active/elemental lithium in your supplement Lithium 20mg? My health care provider thinks it’s 1mg of active/elemental lithium, but it looks like the label says it’s 20mg. Is this the highest amount available in North American market? Could you please also compare your Lithium 20 with Horbaach Lithium Orotate 130mg, in terms which supplements contains more active/elemental lithium? I am attaching the link below. Again, my provider thinks Horbaach contains more of active lithium, but I think it’s the opposite. Please advise. This is very important for us to sort out, so thank you in advance! X.
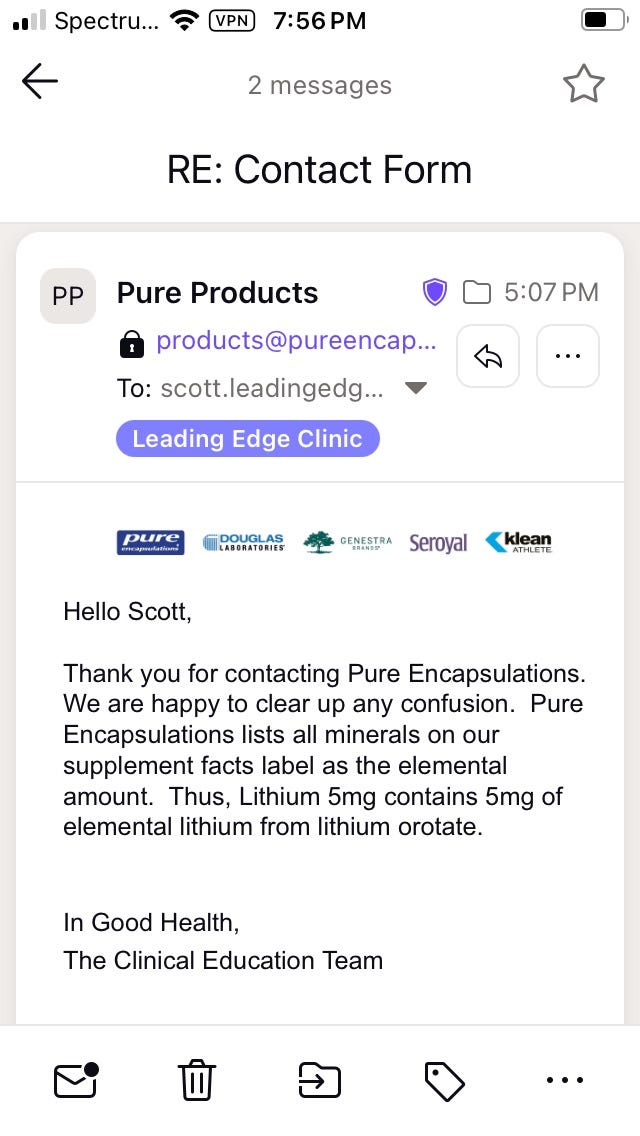
Second, Pure Encapsulations:
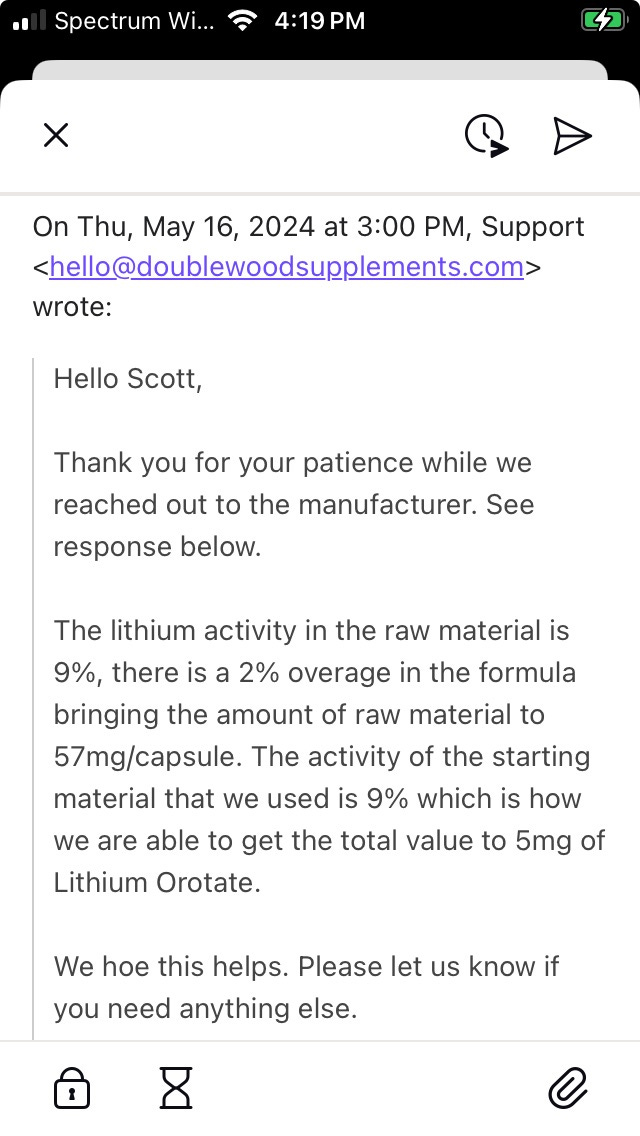
And third, Doublewood. I actually found their answer more confusing. But doing a quick calculation clarifies it. 9% or 0.09 x 57mg of Lithium Orotate = 5.13mg of active Lithium.
Here is my translation:
-
Horbaach delivers 5mg of active Lithium from 130mg of Lithium Orotate
-
Vital Nutrients delivers 20mg of active Lithium from 500mg of Lithium Orotate
-
Pure Encapsulations delivers 5mg of active Lithium from an unstated amount of Lithium Orotate
-
Doublewood delivers 5mg of active Lithium from 57mg of Lithium Orotate
-
Pure Encapsulations also has a 1mg Lithium product, which delivers 1mg of active Lithium, ideal for titration in very sensitive patients.
Clinical reports of symptomatic benefit from our patients indicates that the Vital Nutrients product is either not as effective, or too high a dose in some people. Dr Nehls recommends daily dosing with 5mg of active Lithium for symptomatic patients (active brain fog, neurological symptoms), and 1mg for maintenance. However, we can use up to 40mg twice daily without toxicity in severely symptomatic patients, and so people can titrate under medical supervision.
Normal Lithium dosing for adults with Bipolar disorder is 300-600mg of Lithium Carbonate, two to three times daily, with long-term control using up to 1200mg daily. Lithium Carbonate has 18.78% active Lithium, so that typical daily dosing in psychiatric treatment delivers between 113mg to 229mg of active Lithium. It is for this reason that Dr Nehls writes and speaks of Lithium Orotate as a trace mineral, as 5mg of active Lithium is 4.4% the psychiatric dose, and 1mg is 0.8%. At 40mg daily, which is the highest we have gone in any of our patients, we are still at only 35% of the lowest psychiatric dosing.
P.S. I have no financial interest in any of the supplements which I am discussing.
P.S.S. If you enjoy Lightning Bug, an edition such as this takes at least five hours of my time to conceive, write, and edit. I pay an editor to minimize my typos and deliver a better finished product to you. The recommended annual subscription is $50, but the settings should permit you to make a choice for a smaller amount if you want to demonstrate your appreciation, but like most of us, are on a budget. Please consider becoming a paid subscriber, and share Lighting Bug with others who you think would enjoy it. Peace, Scott
[ad_2]
Source link