The pandemic was rough on us “right-wing anti-vaxxers.” (Who knew being consistently right would be so exhausting?) You might have felt alone at times—but you never were.
Meet your tribe.
Yankee Doodle Soup isa collection of essays by a diverse group of writers with one thing in common: something positive to say about the pandemic. (Really! Those were the rules and the collaborators obliged enthusiastically and expertly.)
Contributors range from well-known doctors and scientists to speakers, podcasters, authors, attorneys, and editors. There’s an Emmy Award-winning former news anchor, a bridal gown designer, a whistleblower, a rock band, and one “pissed-off, childless, married woman of a certain age who didn’t do anything meaningful in her life until [Covid].” The essays are warm, witty, wise, wondrous, and exactly what the world is hungry for right now.
The book was conceived and edited by Jenna McCarthy (co-author of The War On Ivermectin, by my practice partner, Dr Pierre Kory). She has written twenty books, given two TED talks, spoken to groups across the country, served as a staff writer and editor at top women’s magazines in New York and LA, ridden in the back of a pickup truck in a lawn chair, filmed a book trailer in the bathtub, and gone scuba diving with sharks (on purpose). If you ask her daughters her greatest accomplishment, they’d probably say “being interviewed by Khloe Kardashian on the Today show.” Despite this, Jenna would say her daughters are her greatest accomplishment. Yankee Doodle Soup is her first anthology. It may or may not be her last.
Submit your tin foil hat photo to info@bellalunapress.com to be featured in the gallery and for a chance to win a free book!
Please consider buying the paperback or e-book using my contributor code MARSLAND. I contributed an essay titled “Where is God?” Go to https://yankeedoodlesoup.com
Books will ship the first week in June. (That’s when ebooks will be available for purchase as well.) Paperbacks will ONLY be sold through the yankeedoodlesoup.com website, proceeds from which will go to hard working writers like me. Use my contributor code, which is my last name, MARSLAND. If you have enjoyed my Substack, Lightning Bug, over the last six months, please support my work by purchasing this book from the website. Ebooks will be available through Amazon and Apple, with ZERO royalties to the writers.
Most summers I spend a week at the shore in Ocean City, New Jersey. My Aunt Sue and Uncle Bruce generously host. From the time that I was a baby — in fact, when I was still in my mother’s womb — my family would go to Ocean City in the summertime. Bruce and Sue had one, and then two, rental properties there as their working investment towards retirement. There was the huge pain-in-the-ass (PITA) factor of driving down to OC and back through weekend traffic to clean them between renters. Once the PITA grew too large, and the market was looking good, they sold both properties.
Lightning Bug is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
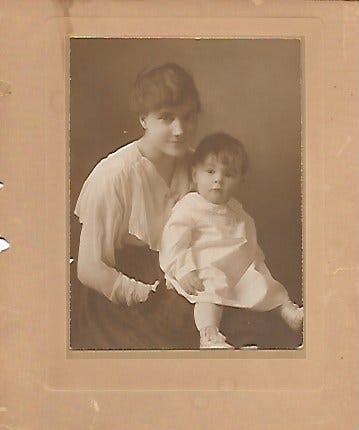
Nana and I, after baptism 1970
Spending time with this branch of the Marsland clan in OC has been a touchstone; seeing my aunt, uncle, cousins, nieces and nephews, catching up on the past year and retelling tales of Marsland lore. When my Nana was still alive, she would be there too, turning a lovely shade of brown while I was working on my sunburn the first few days of sunbathing.
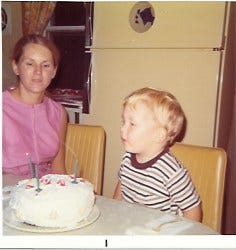
Mom and I, 1972
One of the stories my Aunt Sue consistently retells is that of my mom being pregnant at her wedding to Uncle Bruce. My mother wore a bright orange dress with a short hem, showing off her lovely legs. Beneath the dress, her pregnant belly protruded like a little pumpkin. What I like about that story is that I feel included in the Marsland family history, even before consciousness; I was part of the action, and Sue enjoys reminding me of that.
MORE RECENT PAST
Mom, Sharon and I on Mackinac Island, MI
When I was fourteen, before I ran away to live with my paternal grandparents, my mom and I agreed to take a confirmation class together. My stepfather Em had been a member of the congregation and choir at Christ Church Cathedral, an Episcopal church in downtown Hartford, CT. If there was a church to which we belonged, that was it, but my mom had never been confirmed, and neither had I. For non-Episcopalians in the crowd: confirmation is the opportunity for teenagers and adults to sacramentally and publicly say “yes” to Jesus and His church as expressed through the Episcopal Church. To be confirmed is to be strengthened for ministry by the Holy Spirit and laying on of apostolic (i.e. a Bishop’s) hands. For everyone in the crowd, my favorite saying about being Episcopalian is that we are Catholic light; we haveall the pomp and circumstance, but half the guilt.
Mom and I would commute from our rural abode in Amston, CT into Hartford once a week for months. Ironically, one of the other members of the class was a girl named Karen, an old neighbor from West Hartford days, who I used to tear around the neighborhood with on our Big Wheels. On the actual day of confirmation, there was a service during which the Bishop, who would have been William Bradford Turner Hastings, laid his holy hands on our heads. Aside from Karen and the bishop, I have the gestalt of sharing an experience with my mother in which we were almost equals. It was new, different — and welcome. It was a rare opportunity to see her in another light, as a fellow student and traveler.
PRESENT
Mom in Ithaca, summer 2023
Last summer my mom came for a visit in Ithaca while my wife was away, and we had a lovely time. One of the highlights for me was going on a sailboat cruise up Cayuga Lake with Captain Dave. He grew up in Ithaca, and has been sailing since he was a wee lad. He knows a lot about the history of not only the various structures on the lake, but also the geography surrounding it. The conversation was wide ranging, so of course we got into the topic of the COVID shots and spike protein. Fortunately, that was a side note to the afternoon, as the weather was too glorious, the skies too beautiful, the sails too full, to dwell on such things as we turned southwest to glide back into Ithaca.
Mother’s Day is too easily subjugated by crass commercialism and jostling for position at a crowded Sunday brunch. What I’d like to celebrate today is the imperfection, humanity, and long-term influence of the mothers in my life. Aunt Sue, Aunt Julie, Nana, Baba, Grandma Jones, Grandma Chavez, Betty Ann, my wife (the consummate mama cat), and the woman who gave me life, my mom. Thank you. I love you.
Happy Mother’s Day.
Lightning Bug is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Today I have a facility with numbers and finances, but that wasn’t always the case. When I was a boy, I delivered papers for the New Britain Herald. It was an afternoon paper, back when there were such things. In my substack Capital C Characters, I wrote about the “bionic” man who was one of my customers. I had about 60 customers. Depending on the weather — and how many stops I made for socializing— it took me anywhere from a half hour to an hour to bicycle around delivering their papers after school.
On Saturdays I needed to collect payment. Some customers had subscriptions through the office and mailed in their monthly checks. Most of my customers paid on a weekly basis. I had a little flipbook with tiny, dated coupons that I would tear out and give to the customer when the payment was made. I think this was good practice for life because it meant handling money on a regular basis and, by extension, that means dealing with people’s idiosyncratic quirks around money.
Most customers were home and answered the door on Saturday, knowing I would be there to collect. But there were always a few who either weren’t home or didn’t answer, even though I suspected that they were in there somewhere. This gave me an early lesson in persistence.
Weather in my area of Connecticut at that time could still deliver extreme conditions. Winters were marked by bitter cold and plenty of snow. Flash rain storms with thunder and lightning, gale force winds, hundred degree days with high humidity, not to mention the ferocious dogs that wanted a piece of me: it was all part of the mix. There was one day that I just didn’t feel up to delivering papers and so I didn’t. I delivered Tuesday’s paper with Wednesday’s paper. There weren’t a lot of complaints, but the ones that I did get stung. This was my introduction to providing good customer service while managing extreme dissatisfaction.
At least three times a year my family would leave town on a road trip. This was usually to spend Thanksgiving and Easter with both sets of grandparents in Pennsylvania, and sometimes a week at the shore with the Marsland clan. My parents weren’t micro-managing my affairs, and so this meant that it was up to me to find a substitute to meet my obligations, and pay him well enough that he found it worth his time and effort. This was the upside of my not having helicopter parents. I had to figure this stuff out on my own as early as fourth grade.
Zhivago Velasco and Larry Lebatique became my go-to guys to cover my route. They were both classmates, first generation Americans of immigrant Filipino families. With a memory that astounds me today I was able to easily recall the street names and house numbers for all of my customers and write a list from which Zhivago and Larry could deliver the papers. If I was lucky and most people paid their weekly bill, I would net about $10 a week, which wasn’t bad for 1976. I think that I paid $15 to Larry and Zhivago. I intuitively understood that they didn’t have the relational capital or emotional investment in this enterprise that I did and accordingly I would have to compensate them with more financial reward.
On the other end of things, I would have to hand over the payments to my handler, the nameless adult who dropped off the bundle of newspapers in our driveway six days a week. Every Sunday evening, I would be sitting at the kitchen table with a pencil and eraser doing long addition, subtraction and multiplication to determine the amount of cash and coins I needed to leave in an envelope taped to the storm door for the handler to collect every Monday morning. I never got it right. I never left enough. I tried and tried and tried to understand the formula. I’m pretty sure that I called the main office more than once to try and get some insight. The experience which I had around paying my handler, probably planted the seed for me to become a union agitator and organizer many years later.
What I knew for sure was how hard I worked. And that it felt like I was being cheated. Even worse was that I couldn’t crack the code and challenge my handler, so that his skimming capitalist enterprise could and would exploit my cheap labor. It’s not like I had a mortgage to pay, but I did depend on that money to buy the model planes I liked to build and the candy of which my mother disapproved. I wanted to buy the sugary Fruit Loops and Applejacks cereals that would never make it into our family shopping cart. I even ventured out into more “exotic” cuisine like yogurt, and the stir fried rice from the local Chinese takeout. I acquired an appreciation of the scent of incense from the New Age store, and bought some Phillies blunt cigars, and Malboro cigarettes. So, I continued to ply my trade, knowing that I was being exploited, but was getting some reward that definitely improved my quality of life.
RECENT PAST
When the nuclear power plant at Fukushima, Japan melted down in March 2011, I felt despair which landed on top of my feelings at following the prolonged war in Iraq. I determined that the most achievable and sensible way to counteract that despair was to put solar panels and solar thermal tubes on the roof of our house. My wife certainly didn’t stand in my way, but she never had— and still doesn’t have— the same enthusiasm which I did, which was necessary to pull it off.
We needed to replace the roof around the same time. My wife had been working in construction for 6 to 7 years at that time, co-owner of a small residential building company. Their preferred roofing material was corrugated metal, and some of their customers from the Ithaca community and its environs would install solar panels on their roofs. This meant drilling holes through the corrugated metal which not infrequently led to leaks—and call backs!
At the time, New York State had generous rebates for solar electric, solar thermal, and reflective roofing material. My wife and I are generally inclined to pay more for something that’s built well and will last longer, and we decided that installing a standing seam roof would be the best investment of our money. The racks for the solar panels and tubes could be attached to the seams without compromising the integrity of the roof. Of course, standing seam metal roofs are only slightly less expensive than slate.
We obtained a home equity loan, borrowed more than $10,000 from our stepmother Betty Ann (who took this out of her retirement in order to bridge the expenses until the NY rebates came in) and signed contracts for a roofer and solar installation.
That was thirteen years ago. Given that the roof hasn’t leaked, gas and electric prices have increased exponentially, and the solar thermal tubes paid for themselves by 2019, I think we made a good choice. My wife might still disagree. Her partner in residential construction was very critical in 2011, quipping that “You’ve got a Cadillac sitting on top of your house.” I’m curious, but only slightly, what he would say today.
What I didn’t know back then, but I know now, is that solar electric panels are no bargain for the global economy and environment. The harm to the environment from mining and processing the raw materials to make them, exploitation of cheap labor, and rebates which ultimately serve bigger corporations that finance installation of PV panels on fertile farmland, taking it out of commission… these are all concerning and give me reason to pause.
But let me tell you, when I see neighbors whose 30 year asphalt shingle roof is being replaced after 10 years, I count myself lucky. It gives me great pleasure every time I come down to the basement on a sunny day and see that the domestic hot water has been preheated to more than 100° by the sun. We resell our excess electricity to our utility company. It’s delightful to see the drop in both the charges for supply and generation of electricity sold to us at retail by NYSEG, now a Spanish conglomerate, but retaining its New York name.
These investments would not still be useful if there were not several passionate men who arrived in our moments of need to help troubleshoot and maintain the electricity, plumbing, and various components of these complex systems from which we benefit.
Robert Leroy Nape 1951-2021
It is here that I can write about one of the finest human beings I ever had the pleasure of knowing. Bob Nape and I first met in 2005 when we were both helping to start the Ithaca Free Clinic (IFC). He had serious carpentry skills and together we put up partition walls and drywall to build out the internal exam rooms of the IFC. The thing is that he didn’t just bring his skills, he brought his warmth, humor, and love of humanity, which made it a joy to be around him.
Bob was a man of long-standing passions. He became keenly interested in solar hot water back in the 70s in Philadelphia. He was also an enthusiastic and probably very good basketball player. He certainly had the height and the speed for it. He was more faithful in living his Catholicism and doing good in the world than the Pope, as exemplified by his perspective and actions from the moment he woke every day. Years after we met through the IFC, Bob started his company Solar Is Hot, through which he helped legacy solar thermal systems dating back to the 1970s, as well as newer ones such as ours, remain functional. I cannot take a hot shower without giving thanks to Bob.
We connected around our mutual challenges with heart disease and arrhythmias, which in my case kept me out of competitive sports, but in Bob’s case never kept him from his basketball games. During the pandemic, he developed complications following acute COVID, had a stroke, and ended up at SUNY Upstate, my previous employer. His loving partner Elizabeth, who also helped start the IFC, attended to him faithfully during his last days, and was at his bedside when he died January 2nd, 2021. I count Bob as one of the many great losses of the COVID era, who I think could still be alive today, but for the war on Ivermectin and all repurposed drugs. An odd twist to our story is that when I signed up for a post office box for the Leading Edge Clinic, it turned out that the one assigned, #6834, had been Bob’s.
Another person who has helped us over the last twenty years of home ownership is David, whose last name I don’t know, but who is the constant presence behind the service counter of an old-fashioned plumbing supply business in Ithaca. I have literally carried in a four foot section of twisty plumbing that I cut out of it’s place under our utility sink, and he helped me identify and assemble the new pieces I would need to replace it. He would guide me with patience and humor every time. And so, for good reason, I trusted him.
In September of 2021 our solar thermal system had a problem, and I didn’t have Bob. There was a puddle of the glycol fluid, which was supposed to be circulating in the system, but was instead pooling beneath the expansion tank. Because I didn’t have a choice, I started reading and watching videos, ordered a new tank, and went to David for advice on a fitting. He gathered what I needed from the warehouse, out of my sight, while I waited at the counter. I paid him and drove home to begin my project.
Eight hours and a lot of cussing later, I was unsuccessful. I had depressurized, disassembled, reattached and re-pressurized the new expansion tank six times, and each time there was a leak around the fittings. My kind, loving, patient wife, was trying to have a productive day in her stained glass studio on the other side of the basement, and it wasn’t going well, because as the hours went on, the number of f-bombs coming out of my mouth was increasing.
I had one lifeline which I hadn’t used…Paul Czarnecki, who was mentioned in my Capital C Characters substack. Via phone and text, I explained my predicament, but even Paul couldn’t get me out of this jam. And it was then, after eight hours of blood, sweat, tears and a blue streak of foul language, that I finally understood what went wrong. My dear trusted David had sold me this:
But he didn’t tell me, it was a combination of these two pieces:
As a result, there was not teflon tape or paste between the threads of these two fittings, and under pressure, the connection was leaking. By the time I figured this out, I had put so much torque on the original two pieces that there was not chance of getting them apart, and David’s store was closed. Off to Home Depot I went, purchased the two pieces, came home, wrapped Teflon tape around the joints, reattached the joint and tank, repressurized, held my breath, and turned the circulating pump on again. I swear that on the other side of the wall, my wife was holding her breath too! This time—success— there was no leak!!!!
To this day, that damn fitting sits on my home office desk, to remind me that if we persist and approach challenges with an open mind, questioning our assumptions, we just might sometimes come up with a solution. We just need time to let the little grey cells of our brain work on the problem.
PRESENT
With the author’s permission (my own), I’m going to reiterate part of what I wrote in my subtack Hot Mess Express, in which I discussed the use of Lithium as a trace mineral.
What about Lithium Orotate? Dr Michael Nehls, the neuroscientist from Germany, has been talking a blue streak about Vitamin D and Lithium Orotate to protect our brains from the onslaught of spike. Pierre and I had the pleasure of a private meeting with Dr Nehls nearly two months ago, and he helped us understand that Lithium Orotate was a key tool in the fight to reclaim our brains in general, and the hippocampi in particular. If therapeutics such as Vitamin B6 (as P5P 50), or 5-MTHF, or L-Theanine are useful to rebalance specific neurotransmitters, then Lithium Orotate is a general tonic which helps rebalance all neurotransmitters, because it reestablishes neuronal connections, decreases neuro inflammation, and enables the brain to start making new neurons. The particulars for inidividual patients have proven to be nuanced. I generally start with 130mg, but India Scott FNP-C prefers to start with 20mg of Lithium Orotate and work up to 130mg, stopping if clinical benefit is achieved earlier. Dr Nehls strongly recommended 130mg for symptomatic patients, dropping back to 20-30mg for maintenance when stability has been achieived. It’s important to note that 20-30mg of Lithium Orotate equals 1mg of active Lithium and 130mg of Lithium Orotate equals 5mg of active Lithium.
Because most health professionals — and many laypeople — have preconceptions about Lithium as solely the province of psychiatry and bipolar schizophrenia, it’s important to note that we are talking about Lithium as a trace mineral. Would you be concerned about toxicity from a pinch of Celtic sea salt in your water, or 25mg of Vitamin C? No. Neither should you be concerned about trace amounts of Lithium which are many times less than the doses used in psychiatry. You can get 1mg of active Lithium by drinking a pricey bottle of San Pelligrino mineral water, or eating a lot of seafood, but you’ll also quickly empty your wallet, and in the case of seafood, there are so many toxins in the ocean that you’ll poison yourself with mercury before you reach therapeutic levels of lithium. And it’s cheap, cheap, cheap. Horbaach makes a 130mg capsule of Lithium Orotate which costs $15 a bottle, including shipping, and provides six months worth of the supplement.
The Leading Edge Clinic has several dozen patients in Canada, and together we find ways to get lifesaving supplements and prescription medication to them, in spite of the totalitarian and life-threatening restrictions which the Canadian government continues to impose upon its citizens. Thanks to one of these patients, this week I came to understand that I was somewhat befuddled about the dosing and active Lithium content of the supplements I was recommending. It is my hope to bring light to this topic, as there is ample potential for confusion.
The form of Lithium which Dr Nehls recommends is Lithium Orotate, and that is primarily because of its bioavailabilty and affordability. The trouble begins with how the different supplement manufacturers label their products, and then how the supplement vendors (we use FullScript for a 30% discount for our patients) catalogue the supplements. From my perspective, Horbaach does the best job in their labeling, as the front of the label states “Lithium Orotate 130mg”, and the back states “Lithium 5mg (from Lithium Orotate).” What follows below is correspondence from three other suppliers of essential Lithium as Lithium Orotate: Vital Nutrients, Pure Encapsulations, and Doublewood. First, Vital Nutrients:
Vital Nutrients – Support From:support@vitalnutrients.co To:X Mon, May 13 at 4:42 p.m.
Good afternoon,
Thank you for contacting Vital Nutrients.
There is 500mg of total lithium orotate and 4% is elemental. So 20mg of elemental lithium and 480mg of orithic acid. (for round number purposes)
This is the highest we do carry. We are unable to do a comparison as other companies may source raw materials from other vendors. It would not be an accurate comparison.
If there is anything else we can do today, please let us know.
Omar Customer Care Representative II 888.328.9992 | vitalnutrients.co
On Mon, May 13, 2024, at 08:41 PM, X> wrote: To follow up on my previous question…I think the confusion has arisen from the fact that it doesn’t say Lithium Orotate on the front of your bottle, just Lithium. So I read it as 20mg of pure lithium. If it’s not correct, and 20mg is the amount of lithium orotate, then what is the actual amount of pure/elemental lithium in your supplement? If the opposite is true and 20 mg is the amount of pure lithium, what is the amount of lithium orotate per capsule?
On Mon, May 13, 2024, at 08:29 PM, X> wrote:
Hello, could you please confirm the amount of active/elemental lithium in your supplement Lithium 20mg? My health care provider thinks it’s 1mg of active/elemental lithium, but it looks like the label says it’s 20mg. Is this the highest amount available in North American market? Could you please also compare your Lithium 20 with Horbaach Lithium Orotate 130mg, in terms which supplements contains more active/elemental lithium? I am attaching the link below. Again, my provider thinks Horbaach contains more of active lithium, but I think it’s the opposite. Please advise. This is very important for us to sort out, so thank you in advance! X.
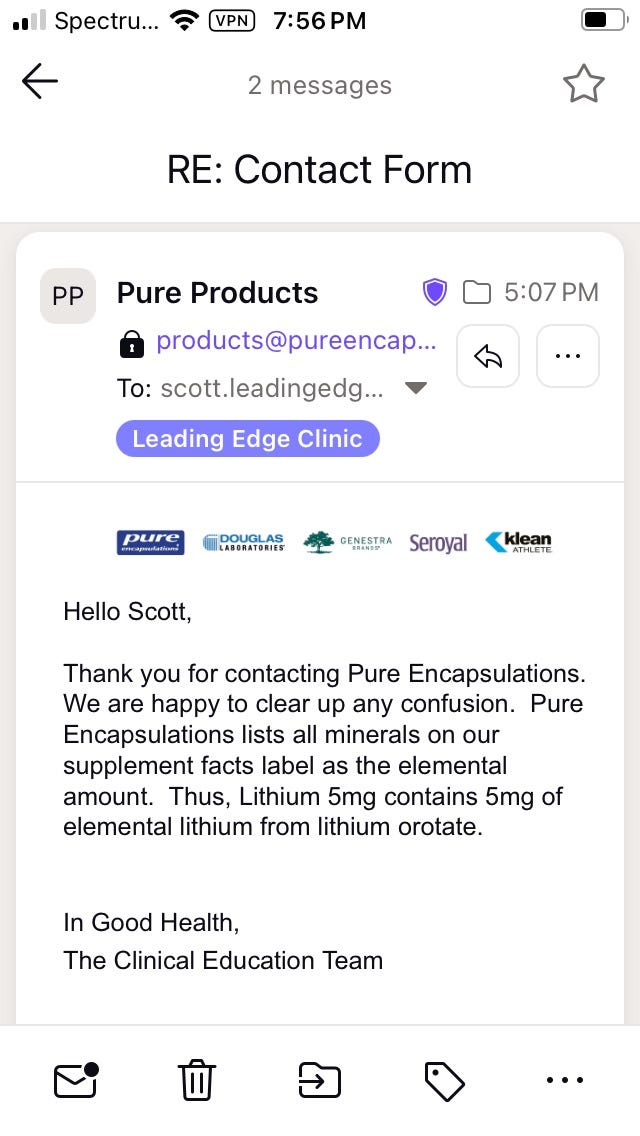
Second, Pure Encapsulations:
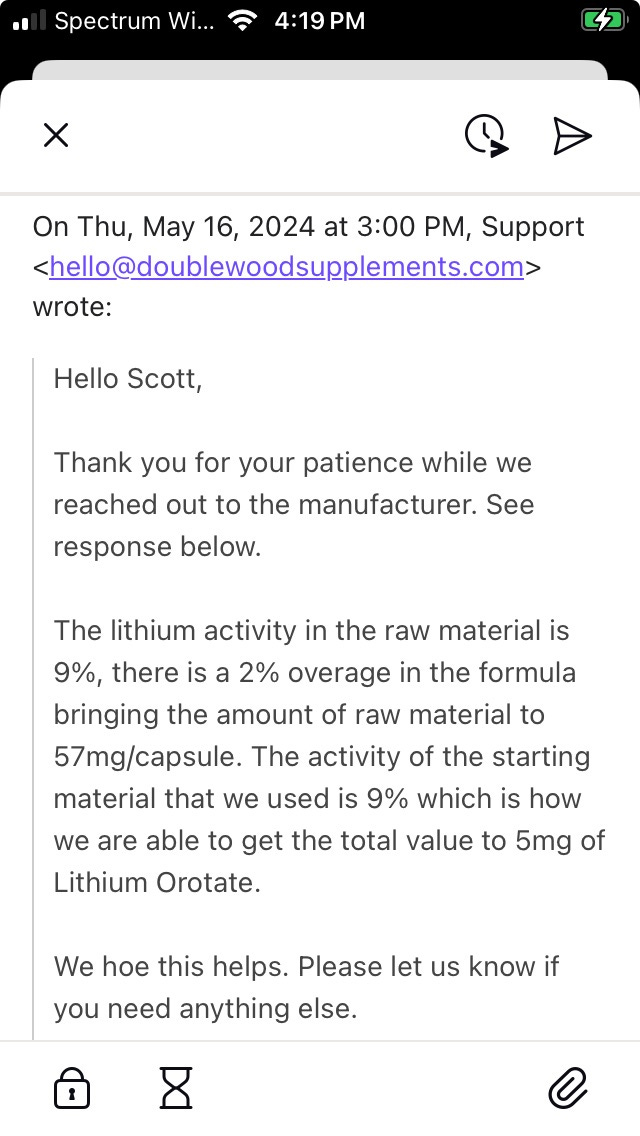
And third, Doublewood. I actually found their answer more confusing. But doing a quick calculation clarifies it. 9% or 0.09 x 57mg of Lithium Orotate = 5.13mg of active Lithium.
Here is my translation:
Horbaach delivers 5mg of active Lithium from 130mg of Lithium Orotate
Vital Nutrients delivers 20mg of active Lithium from 500mg of Lithium Orotate
Pure Encapsulations delivers 5mg of active Lithium from an unstated amount of Lithium Orotate
Doublewood delivers 5mg of active Lithium from 57mg of Lithium Orotate
Pure Encapsulations also has a 1mg Lithium product, which delivers 1mg of active Lithium, ideal for titration in very sensitive patients.
Clinical reports of symptomatic benefit from our patients indicates that the Vital Nutrients product is either not as effective, or too high a dose in some people. Dr Nehls recommends daily dosing with 5mg of active Lithium for symptomatic patients (active brain fog, neurological symptoms), and 1mg for maintenance. However, we can use up to 40mg twice daily without toxicity in severely symptomatic patients, and so people can titrate under medical supervision.
Normal Lithium dosing for adults with Bipolar disorder is 300-600mg of Lithium Carbonate, two to three times daily, with long-term control using up to 1200mg daily. Lithium Carbonate has 18.78% active Lithium, so that typical daily dosing in psychiatric treatment delivers between 113mg to 229mg of active Lithium. It is for this reason that Dr Nehls writes and speaks of Lithium Orotate as a trace mineral, as 5mg of active Lithium is 4.4% the psychiatric dose, and 1mg is 0.8%. At 40mg daily, which is the highest we have gone in any of our patients, we are still at only 35% of the lowest psychiatric dosing.
P.S. I have no financial interest in any of the supplements which I am discussing.
P.S.S. If you enjoy Lightning Bug, an edition such as this takes at least five hours of my time to conceive, write, and edit. I pay an editor to minimize my typos and deliver a better finished product to you. The recommended annual subscription is $50, but the settings should permit you to make a choice for a smaller amount if you want to demonstrate your appreciation, but like most of us, are on a budget. Please consider becoming a paid subscriber, and share Lighting Bug with others who you think would enjoy it. Peace, Scott
Helen Boyd Marsland and Walter Stanley Marsland, Jr (my Pop pop)
PAST
A refrain which I heard frequently as a child was that I was “just looking for attention.” I had some intuition that this wasn’t a bad thing, but it was framed as just that by some of the adults around me who had other interests besides paying attention to a little boy.
Fortunately for me, there were other adults who were happy to pay attention. This included dozens of grey and white-haired customers on my paper route, my paternal and maternal grandparents, and my godparents. There was enough collective attention among them that I emerged from childhood without getting picked off by some predator who could smell the attention-starved boys and girls like a fox smells the rabbit.
When I was fourteen years old, my friend Larami’s parents sponsored me to go to a weekend workshop for young people. It was my first introduction to Re-Evaluation Counseling or RC, was held in a big old house in West Philadelphia, and led by an RC leader named Blair Hyatt. Larami was there too, as was another high school classmate named Tracy, and about a dozen other teenagers. That weekend changed my life, and how I thought about people—and attention.
The way these workshops go, each person gets a turn, if not multiple turns, in front of the group with the leader paying attention to them. Even the leader takes a turn. This last piece is important, because, unlike most conventional therapies in which the therapist is positioned as the knowing one, within RC, the leader has the opportunity to share their struggles with their community. It’s a different model of leadership, which has pluses and minuses, and doesn’t necessarily translate to the non-RC world.
One thing which I learned that weekend was that no matter how confident and together someone looked on the outside (e.g. Tracy), everyone had an interior emotional life, insecurities and old hurts that they were handling. This became clear to me as we took turns listening to each other in small groups as well as the entire group. The stunning moment was when Tracy was in front of the group with Blair paying attention to her in a light and playful way, and she burst into tears. I remember thinking, “What the hell just happened?” I didn’t expect this, and somehow the attention of Blair and the group made the difference. Tracy showed herself in a way that I hadn’t seen in the two years I had known her, and it made me care more deeply about her.
Another very important thing which I learned that weekend was that we all want and need attention, but that things go much, much better if we take turns. This immediately made sense to me. How many times have we been in a conversation where everyone is chomping at the bit to speak, and not necessarily listening to what the other people are saying? RC explicitly circumscribed this approach, by using timers, with each person taking a turn as client and counselor. You could begin to let go of formulating what you wanted to say while someone was still speaking, because you knew that your turn would come.
Perhaps the most important thing I learned that weekend though, was that I was a good listener, and that my listening could help another person to heal. People at that workship, and in RC over the years, showed me how to use attention to examaine what has been hard in life, with the aim of moving through it and moving on from it. I felt like I had discovered a superpower. We all have a need to be loved, but I would assert that our need to demonstrate our love for others, is far greater. RC presented me with a way to do this regularly, and skillfully.
RECENT PAST
One of the best decisions I ever made was to get a vasectomy in my mid-twenties. (I didn’t yet know that vasectomies don’t prevent you from adopting large numbers of cats, but that is a story for another day). For a year and a half I had been living together with the woman who would become my wife. I was still swearing that I would never get married, but was even more certain that I didn’t want to have children. She wasn’t as fervent on the issue of kids, but we both had come from broken homes, and had serious doubts about our capacity to be good parents. And so we came to an agreement that I would get fixed. So out-of-the-norm was this desire, that it took another year for my primary doctor to agree to sign off of the surgery, as he wanted me to take a year to “think about it.”
At this point in life, I don’t doubt that my wife and I could be good parents, if only because we have spent so much time raising each other into adulthood, and becoming relatively balanced human beings. But I’m still glad that we didn’t become parents. What we have had as a child-free couple is fewer financial constraints, more time, and freedom.
Parenthood doesn’t have to be the death of romance in coupledom, but it sure seems to be a common side effect. You can read romance to mean not just a sex life, but also closeness, connection and a fighting chance at finding intimacy, whatever that elusive relational state may be for you.
Wally and Devon 1999 (a sketch by my sister-in-law Carolyn, of my father, frail and nearing the end of his life, with our middle niece Devon)
As a child-free couple, we have been able to step up during some very important times in the lives of our extended family. When my sister-in-law was in the hospital for a major surgery, I was able to take time off from work to help watch my three nieces while my brother worked long hours at a demanding job in finance. When my father was dying of metastatic kidney cancer, we were able to regularly drive five and a half hours to his home, and provide respite to my stepmother during the last months of his life. We did this at a time that we were both working retail jobs, didn’t have a car (we would rent one) and with finances that were very tight. When my paternal grandmother was dying from colon cancer, and had burned her bridges with my aunts and uncles, we were able to take her into our home and care for her during her last month of life. Each of these experiences was deeply meaningful and had its own intrinsic rewards for us, but I know also made a big difference for those receiving our time and attention.
Niece Kayla and Uncle Scott
My wife learned RC when we first moved in with each other in 1994, and quickly became a skillful counselor, better than me in fact, even though I had been at it a decade longer. We tried to use our super powers of attention to elevate the emotional lives of our nieces and nephew. We’ll never know what impact those efforts had, but we quickly understood the limitations of our influence, as parents often seen their children as their private property, and can quickly perceive competition and threat from other adults who have relaxed attention for them.
One summer we had two of our nieces come to visit us in Ithaca, NY and had a memorable week hiking, camping, and exploring together. My brother and sister-in-law expected the girls to be homesick, and were miffed when they didn’t get a call which affirmed this. The week was not without its challenges, as our nieces tested us and used our attention to show some of the struggles they had, but couldn’t get air time on at home. I think that all of us had a sense of closer connection to each other by the end of the week, and my wife and me were looking forward to another visit the next summer. When we later asked about having the girls come visit again the next summer, we were told that they would be going to camp. I suspect we did not get that opportunity again because my brother and sister-in-law perceived a threat to their parental exclusivity and validity.
Given what I have learned about attention, giving and receiving, and the healing power of it, I’ve long thought that many people shouldn’t become parents, or at least not as soon as they do. All humans need attention, but children especially. How rational is it that people become parents when they haven’t developed their capacity to pay attention to others? As far as I can tell, good parenting is more likely to flow from adults who have some capacity to meet their own human needs, including self-validation, without needing to extract it from the dependent little creatures they brought into this world. I have come to believe that developing our capacity to pay and share our attention can only improve our interactions with each other, and the children in our lives.
PRESENT
As a Family Nurse Practitioner, I was trained in delivering care to human beings from birth to death. If I had to, I think that I could do a decent job of delivering a child, but I’d rather not. I’ve cared for plenty of children during years of work in an Emergency Department which treated children and adults, but pediatrics isn’t my favorite. Yet, due to the uniqueness of thess post-Covidian time, there have been teenagers and pregnant women who have needed my care.
The most frequent appearance of pregnancy in my practice with the Leading Edge Clinic has been after a miscarriage or stillbirth. Women and couples who are seeking to understand what about COVID or the COVID shots is interfering with successful pregnancies seek out our counsel. I think that we have some insights into the pathology of the spike protein which have been helpful in those cases.
In one instance, a young woman who had started treatment for injury from the COVID shots, was due for a second visit, and became pregnant in the interim. During our second visit, I met with this patient and her husband, and the focus was on how we should modify her plan of care now that she was pregnant, and specifically, whether or not she should keep taking Ivermectin.
Medicine is perpetually an enterprise of risk vs benefit. What we witnessed in the last four years was the utter abandonment of informed consent, which cannot occur in any meaningful way without discussion of risks vs benefits of different treatment options. In discussing the use of IVM with this couple, I explained that there was some evidence of teratogenic effects (birth defects) of IVM in the first trimester, but at doses which were also harmful for the mother. We have been treating patients with IVM since February 2022, and I haven’t seen worse than blurred vision or GI upset in a minority of patients, despite doses as high as 0.6mg/kg. (There were two patients who were self-described as very sensitive to everything, who had what I would describe as Herx reactions upon initiation of IVM dosing, even at 1mg per day, but they were extreme outliers).
This particular patient had stopped IVM when she learned that she was pregant. She was taking only 2mg per day, which is far lower than I use in most patients, but she was also a self-described sensitive patient. Within three days of stopping IVM, the symptom of dizziness which had been plaguing her prior to taking IVM, returned.
To counterbalance our discussion, I asked the rhetorical question: “Have you been told that it is safe to take Tylenol (Acetaminophen) in pregnancy?” Yes, they had been told that it was safe. I then relayed my understanding of acetaminophen’s safety— or lack therof. For purposes of this Substack I’ll stick with the less impressive, but also less debatable numbers. According to the CDC, 1567 people have died from accidental Tylenol overdose between 2001-2010. During that same time period, annual acetaminophen-related deaths amounted to about twice the number attributed to all other over-the-counter pain relievers combined, according to the poison control data. A 2018 study published in a Scandinavian journal reported acetaminophen poisoning was associated with increased long-term all-cause mortality. The increased all-cause mortality was more prominent in the younger population, and in the first 12 months after poisoning. In July of 2009, an FDA panel of thirty-seven experts came very close to issuing a call for a ban on all over-the-counter sales of acetaminophen to reduce associated deadly overdoses and to eliminate the leading cause of liver failure in the U.S. They instead pulled back and called for only limiting the amount of Tylenol used in combination with narcotics such as Percocet. A 2023 study found that this decision saved many lives. This 2013 report from ProPublica does a good job of chronicling the sordid and deadly history of acetaminophen, and Big Pharma’s dodginess in response to decades of efforts to curtail its over-the-counter availability and use. However, it is still widely considered safe to use in pregnancy.
Now, let us again consider IVM. In 2021, a French company which had developed a long-acting, injectable form of IVM, commissioned a sweeping study of the medical literature on IVM by the well-respected French Toxicologist, Dr Jacques Descotes. He examined 82 chapters in multi-authored books, 249 original scientific papers, 74 review papers in peer-reviewed journals, 486 presentations and posters at scientific meetings on the preclinical and medical safety assessment, immunotoxicology and immunological safety, regulatory safety and risk evaluation of medicinal products and chemicals. In more than three decades of use, in hundreds of millions of people, there wasn’t even a solid case to be made that IVM was associated with a single death. He concluded that “…the safety profile of ivermectin has so far been excellent in the majority of treated human patients so that ivermectin human toxicity cannot be claimed to be a serious cause for concern.”
I know which of these two products I would feel comfortable recommending for use in pregnancy.
A 2020 systematic review funded by Unitaid (read Bill Gates) found: “There is insufficient evidence to conclude on the safety profile of ivermectin during pregnancy. Treatment campaigns should focus additional efforts on preventing inadvertent treatment of pregnant women.” I find it noteworthy that the recommendation is to prevent inadvertent treatment rather than more closely study its safety in pregnant women, and the authors take pains to point out the low quality of the studies used.
No evidence was found for increased risk of neonatal deaths, preterm births or low birthweight. Some evidence was found for spontaneous abortions, stillbirths, and congenital anomalies, but the number of cases was too low to be conclusive – fewer than 100 women were exposed during the first trimester, when the foetus is expected to be more vulnerable to the drug’s effect.
Alternately, in its discussion of the Unitaid (Gates) review, the Barcelona Institute for Public Health spends a moment longer on the pertinent point that if IVM could be shown to be safe in pregnant women, that would be very important for public health. That is because IVM is not only used to treat the parasitic infections of onchocerciasis, lymphatic filariasis, Strongyloides, and scabies, but also has potential role as an endectocide to reduce malaria transmission by killing malaria vectors. The consensus of scientists and public health workers is that malaria kills up to 2.7 million persons each year. Nine out of ten of these cases and deaths occur in Africa and the vast majority of them are in children under the age of five years. If IVM got the green light for use in pregnancy, it could save many more lives.
The introduction to the Unitaid (Gates) review is worth quoting in detail; highlights are mine.
Before moving to the narrative description required by the 2015 labelling rule,9the US Food and Drug Administration (FDA) had previously classified ivermectin as pregnancy category C—ie, “Animal reproduction studies have shown an adverse effect on the foetus and there are no adequate and well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks”.1 This classification is based on studies done in mice, rats, and rabbits during the original New Drug Application in the 1990s by Merck (appendix p 2).10These studies showed adverse pregnancy outcomes at cumulative doses that are high enough to produce signs of maternal toxicity in animals, ranging between 20 and 600 times the human Mectizan single-dose target of 0·15–0·20 mg/kg. However, later evidence showed that the mouse strain (CF-1) used in the initial acute and developmental ivermectin toxicity studies was inappropriate, as it was later shown that CF-1 mice have deficient P-glycoprotein expression, which is an efflux pump key to preventing ivermectin toxicity.11
My interpretation of the above is as follows. First, if we were to dose a pregnant human female at 20 to 600 times the typical single-dose use of 0.15-0.20mg/kg, for a 120lb (54.5kg) woman, instead of 12mg, we would use doses of 1090 – 6540mg. That ain’t happening. Second, the mouse studies which demonstrated teratogenicity to the fetus used a type of lab mice which have a genetic mutation that leaves them unable to avoid IVM toxicity. Hmmm.
I’ll report that in our clinical experience, whether a person has received the COVID shots or not, all of our patients have amyloid fibrin microclotting. If a person received two or more shots, they will typically have microclotting stage/grade 3-4 on a scale of 0-4. We know that microclots concentrate in the capillaries, where red blood cells (RBCs) are meant to deliver oxygen and remove carbon dioxide, but can’t due to congestion and blockage. We also know that the dense networks of blood vessels within the placenta are responsible for exchanging respiratory gases, nutrients, and wastes between the mother and fetus throughout pregnancy, which is essential for proper fetal growth. And we know that IVM is very effective at blocking the clot- provoking impact of spike on the platelets, RBCs, and endothelial cells which line the blood vessels.
In a post-Covidian world, the risk of using IVM in pregnancy is inhibited by the inconclusive and weak body of evidence (per Unitaid (Gates)), and studies using mice which couldn’t avoid IVM toxicity at crazy high doses. On the other hand, we have a punctilious review by an esteemed toxicologist, basically saying that IVM hasn’t killed anyone over thirty years and hundreds of millions of doses. And our clinical experience reveals microclotting in everybody, which poses an imminent threat to the viability of a fetus. IVM is one of the most effective therapies to block that effect of spike to promote microclotting.
If it was my wife who was pregnant, after a detailed review of the above risks and benefits, I would opine that I think the risks of IVM at current dosing at 0.2mg/kg-0.6mg/kg for post-acute sequelae of COVID and COVID vaccine injury are not only safe in pregnancy, but likely to prevent fetal demise from microclotting. If my wife was especially sensitive and cautious, I would use as little as 1mg of IVM daily, but I would use it.
P.S. This Substack is not individual medical advice for you.
P.S.S. Happy Memorial Day!
P.S.S.S. Thank you to each of the paid subscribers who help support the long-term effort of writing.
This story takes us back to my adventures with the Brethren Volunteer Service (BVS), as recounted in Hot Mess Express. After my excommunication from the San Antonio Catholic Worker House, I became sick as a dog for a week. Physically recovered, I flew home to southeastern Pennsylvania and stayed with my Nana. For the next week she was loving, but firm and clear that she wasn’t going to tolerate a twenty one year old college graduate who was a failure-to-launch. She had spent too many years watching the shenanigans of the neighbor biker boy Donny who was still living with his mom and dad—in his forties!
In the meantime, the BVS decided to give me a second chance. The High Desert Ranch in New Mexico had decided that I was indeed a hot mess, and retracted their acceptance. But, there was a Church of the Brethren (COB) camp and retreat center in Hooversville, PA which would be glad to have me. Hooversville is a tiny hamlet in Southwestern, PA, and Camp Harmony was miles from the nearest neighbor, a dairy farm. The position was for a Maintenance Director, with on-the-job training.
And so I arrived in the middle of Winter via Amtrak from Philadelphia’s 30th Street station. Philadelphians tend to think that Pennsylvania is, well, Philadelphia. The fact that the state extends at least an eight hour drive westward, and has a snow belt in the southwest to rival midwestern winters was not part of this southeastern Pennsylvanian’s consciousness.
The Winter and Spring were long and lonely. There was a lot of work to do on the buildings and around the camp preparing setting up for weekend retreats and preparing for the summer. During the weekdays, the camp secretary and director would be in the office and available, but at night I was the only person for miles. The upside was seeing the starry sky in all its heavenly glory and without the light pollution from the city. 1992 was also a heyday for country singer Garth Brooks, and considering that the only radio reception I got was AM, and two stations—both country—it was a good thing. I learned to like country music out of necessity.
Sundays meant traveling with the Camp Director, Neal Harvey, to regional congregations of the Church of the Brethren to make a presentation about the camp and raise funds. Neal would play a recording of campers singing the folk standard “The Garden Song” —listen to this version by John Denver appearing on The Muppet Show. It was an ear worm and still lingers in my brain on the occasion that I think of Camp Harmony….
As the snow began to clear, Wednesdays were work days with a group of up to ten retired men. We cut down Black Locust trees to make new fence posts and strung them with barbed wire to keep the neighboring cows off the camp property. We also began clearing land to make way for a planned new retreat center, today known as Faith Hall. All of this involved a lot of work with an old John Deere tractor, and chainsaws, neither of which had been part of my upbringing.
We took care, and no one was hurt during out efforts—except for one incident. Howard Fyock was a retired “coal cracker”, Pennsylvanian for coal miner. Like many old time coal miners, he had black lung. Coal workers’ pneumoconiosis (CWP), commonly known as “black lung disease,” occurs when coal dust is inhaled. Over time, continued exposure to the coal dust causes scarring in the lungs, impairing your ability to breathe. Considered an occupational lung disease, it is most common among coal miners.
I shit you not that Howard would be out there driving the old John Deere with his oxygen nasal cannula and the accompanying portable tank slung from his shoulders. There was an old gravel pit which we would dump the huge stumps we had dug out as we cleared the land. One day, Howard had the bucket end of the tractor elevated, with a large stump suspended below from a chain. As he approached the top of the gravel pit, there was a little too much swing to the stump, left to right, and the bucket was elevated just high enough that physics took over and the tractor began to tip. What happened next remains a marvelous miracle, and testimony to Howard’s quick thinking and spryness, even at the age of 80. He leapt off the tractor, in the opposite direction from which it was rolling, with his oxygen tank no less, and cleared the moving machine before it could crush him as it cartwheeled fifty feet down into the pit.
Neal and I visited Howard later that day in the hospital, and aside from some extensive bruising and a few broken ribs, he was already agitating to be discharged. The John Deere was also banged up, but after a visit to the shop to straighten out the engine splash guard and replace the damaged hydraulic lines, it was back in action.
I remember Howard and the other men who volunteered every week with a swell of love in my heart. Being a decent cook, I tried to show my appreciation for them by eschewing the basic fare of sandwiches, chips and iced tea, for more complicated and filling meals such as lasagna with garlic bread and salad, or chili with cornbread. Neal raised an eyebrow about the added expense, but that didn’t squash my light. He had a decent appetite himself, so I’m sure that helped.
When summer finally arrived, so did a whole community of staff and counselors, followed shortly afterwards by the campers. I had to surrender my apartment to the camp nurse, and move down to the lodge used for staff; those quarters had women on one side, men on the other, with a common room and kitchenette in the middle. Some of the lodge’s residents were still minors and as a result, even though I was what in Philadelphia street language would be called “a grown-ass man”, I was now theoretically under the nightly curfew watch of the camp nurse, with the young‘uns.
Always on the lookout for love and romantic adventure, I became friendly with one of the kitchen staff, a pretty young lass named Dawn. We managed to have a nice snuggle on the couch in the common lounge without any objections from our peers. What I hadn’t counted on was the late arrival of a camp counselor from Russia. Her name was Julia Samsonova, pronounced sam-Soo-no-va. We had eyes for each other from the start, with hers being dark, penetrating, and conspiratory.
Julia back in Russia 1993
About a week after Julia arrived, we ended up in the common lounge together one evening; she asked if I could play chess. Yes, indeed I could—badly, but I’d give it a go. It was unlike any chess game I have ever played, before or since, with the banter, saucy looks and a rising tension that left me so stirred up that I could hardly get to sleep that night. But what is a guy to do in the middle of a Christian summer camp, under the watchful eye of the camp nurse? Try to behave; try being the operative word.
I would leave you hanging if I didn’t share one last bit. Despite Neal’s generosity of heart in taking a chance on my hot mess and offering me a volunteer position, at the end of the summer I left Camp Harmony, and my volunteer commitment, early. There were a number of factors which, combined, led to this decision. It turned out that this region of the Church of the Brethren was more fundamentalist in nature, and I struggled with that. I also thought that volunteer doesn’t equate to servant, and Neal’s expectation of my position was that I would work 60-80 hour weeks throughout the summer, because previous volunteers in my position did. I have a strong work ethic, but this felt like exploitation of my good -faith intention to serve, and that didn’t sit well with me. I needed to move on.
The morning that I left Camp Harmony, Neal’s wife Karen had come to pick me up to take me to the train station. At the same time Julia was sneaking out of the window of my room and headed around the side of the staff building, Karen arrived at the front door and they made eye contact. Ooops. Karen wasn’t dumb, and put two and two together. I later learned that this news scandalized the COB community and, typical for small town gossip, lead to quite the storm of grandiose stories about how the Devil had influenced me, corrupted Julia and who-knows-else and who-knows-what. After we briefly considered her coming to Philadelphia to join me, Julia headed back to Russia. I wasn’t anywhere near ready for marriage, and the daunting logistics of obtaining an extended visa were enough to end our romance.
RECENT PAST
Russia House #1 in California
In 2018, my wife and I traveled to California to visit her father and his wife. Curt and Jane were high school sweethearts, who reunited after more than twenty years, several children each, and divorces from their respective spouses. They had recently purchased a large RV trailer and we took a small trip together to the coast, traveling through the Russian River Valley. On our way to the coast, we passed Russia House #1 and it caught my attention. It was an odd-looking structure which sat near the edge of the Russian River, with a sign advertising traditional Russian food. I filed it away in my head and, on the return trip, I asked Curt to pull over so that we could check it out.
When we pulled into the parking lot, there were no other cars, and when we entered the building, there were no other people. Just inside the entrance there was a room with an eclectic collection of puzzles and games. Further in, there were several large tables laid out with at least a dozen large crock pots, plates, and silverware. After a few minutes wait a rumpled-looking fellow came out from the back and introduced himself as the neighbor from across the street. He was watching over things as the three women who sponsored this culinary experiment were away for the day. He explained that we help ourselves, buffet-style, eat as much or as little as we want, and pay what we think makes sense. Hmmmm. What was the catch? I was both surprised, and a little suspicious, but when I read one of the postcards on our table, I started to understand what this was about.
Russian house#1 is a free cultural space, intentional community and an experiment in new economics. Russian House #1 is a unique Restaurant, where the food is being served like at Home. It means that we do not have menus, nor fixed prices. Our food is being prepared with an inspiration every day, considering our favorite Russian recipes and healthy local produce. We do culinary classes and we love to take best cooking practices from our guests. (Yes! You are welcome to cook with us or to cook for us ))) We have a great puzzle collection, intellectual clubs, meditations and breath work workshops .”
A view from the restaurant. (Polina Krasikova/Russia House #1)
Everything smelled and tasted delicious, and some the food was familiar due to commonalities between Russian cuisine and Slovak dishes which my Baba would make. It was homemade Russian peasant food: hearty soups, stews, blini and salads were presented on a buffet table. Tea, fruit drinks and water were also available. The view of the Russian River Valley was lovely. Yes, I went back for seconds. I was grateful that my travel companions were willing to take a chance and explore this very special place together, and they all seemed to enjoy the food as well. I think I left $100 to cover the four of us.
President/Manager Tatyana Urusova, left, with co-founder Polina Krasikova, volunteer Maura Dilley and co-founder Tatiana Ginzburg. (Russian House #1)
Researching for this Substack, I learned that Russia House #1 closed in January of 2022, when the landlord declined to renew their lease. I’m betting that the inspired Russian women behind this culinary/intellectual/spiritual/diplomatic experiment will re-emerge in another location to continue their adventure. If you’re interested in more details, Russia House #1 was covered in these 2021 Washington Post, 2022 San Francisco Chronicle, and 2022 The Press Democrat articles.
PRESENT
Besides my Russian love Julia, and the yummy food of Russia House #1, I was inspired to write this Substack by my observations regarding a drug called Sulodexide. The only way I know of to procure this drug is via what I’ll call the “grey market,” as it is not available in the U.S. On websites which change from week to week, using similar graphics but different names for their business, people with names like Igor, Boris, Alexsandr and Dimitri bridge the gap between individual medical needs and the stupid greed of our Pharma-compromised FDA. I mention this at the start, because, as you will see, Sulodexide is not for the faint of heart, pardon the pun, as you will see.
What is reassuring about Sulodexide is that is has been approved by the European drug agencies and has been in use since 1972. When a drug has a long history of use, there has been plenty of opportunity to explore it’s pluses and minuses. Sulodexide is available as a generic medication, which makes it cheaper than comparable drugs such as Eliquis, an anticoagulant which is a factor Xa inhibitor. Eliquis has a good safety profile, and in our use of it to treat micro clotting-for more than 500 of our patients , there have been very few complications. However there is evidence that Sulodexide is safer than Eliquis. I would argue that it being cheaper and safer than Eliquis makes it very unlikely that we will see Sulodexide approved by the FDA anytime soon, as it would threaten the Pharma profits from Eliquis, Xarelto, and similar patented drugs.
Why am I talking about Sulodexide? First, the sheer scope of sulodexide’s clinical effects: it has anti-atherosclerotic, anti-coagulative, anti-fibrotic, fibrinolytic, anti-inflammatory, and endothelium-protecting properties. Second, I have seen noteworthy improvements in the symptoms of two vaccine injured patients who used a one month treatment of Sulodexide with 250LU (25mg) twice daily. I diagnosed the first patient with iliac venous compression (IVC). She took Sulodexide for one month before she had stenting with my colleague Dr Brooke Spencer in Denver, CO. She was noting improvement even before the moderate sedation was wearing off, and, among my growing list of IVC patients, has experienced one of the most rapid and dramatic improvements in her vascular system, chronic back pain, energy, and cognition. The second patient took Sulodexide for one month, and while he didn’t notice any tremendous benefit while taking it, his long-term recovery has been exemplary, as he has steadily improved in his reports re: ease of breathing, absence of chest pain, increased exercise capacity, and overall well-being.
Sulodexide (SDX), a sulfated polysaccharide complex extracted from porcine intestinal mucosa, is a blend of two glycosaminoglycan (GAG) entities, namely a fast-moving heparin (HP) fraction and a dermatan sulfate (DS; 20%) component. The compound is unique among HP-like substances in that it is biologically active by both the parenteral and oral routes. A main feature of the agent is to undergo extensive absorption by the vascular endothelium. For this reason, in preclinical studies, SDX administered parenterally displays an antithrombotic action similar to that of HPs but associated with fewer alterations of the blood clotting mechanisms and tests, thus being much less conducive to bleeding risk than HPs. When given orally, SDX is associated with minimal changes in classic coagulation tests, but maintains a number of important effects on the structure and function of endothelial cells (EC), and the intercellular matrix. These activities include prevention or restoration of the integrity and permeability of EC, counteraction versus chemical, toxic or metabolic EC injury, regulation of EC–blood cell interactions, inhibition of microvascular inflammatory and proliferative changes, and other similar effects, thus allowing oral SDX to be considered as an endothelial-protecting agent.
So, Sulodexide has two components, or fractions. The low molecular weight of both sulodexide fractions allows for extensive oral absorption compared to unfractionated heparin. The pharmacological effects of sulodexide differ substantially from other GAG drugs and are mainly characterized by a prolonged half-life and reduced effect on global coagulation and bleeding parameters. Translation: with Sulodexide there is less risk of bleeding.
We understand from our study and treatment of patients with post-acute sequelae of COVID and injury from the COVID shots, that endothelial (cells lining the blood vessels) injury occurred when the spike protein entered the blood and circulated. This happened to an exponentially greater extent from the shots, but can also occur in people who have had COVID, or who are experiencing shedding from exposure to vaccinated and boosted individuals. Therapeutics such as Sulodexide, which can counteract this endothelial injury, could be very valuable.
Sulodexide has been studied extensively in relation to venous ulcers, chronic venous disease, and diabetic neuropathy. There was one study of Sulodexide use in PASC patients with chest pain, which had positive statistical and clinical significance. One application which intrigues me, and which I will be exploring with patients, is its potential use in treating tinnitus, because that has been one of the hardest nuts to crack in PASC and vaccine injury. Sulodexide studies showed that when used in conjunction with melatonin, or as monotherapy, it was a viable treatment option for patients suffering from central or sensorineural tinnitus.
I expect that this brief exposition on Sulodexide will raise more questions among readers. Please remember that this is not individual health care advice for you. If Sulodexide sounds promising to you, please do more research on your own, as there are many academic articles to be found, and discuss it with your healthcare provider. I suggest starting with PubMed, the free online search engine available through the NIH. As with purchasing other medicine, such as IVM, from outside the United States, there are inherent risks which the regulatory structure of FDA approval is meant to protect us from (but which can also impede our access to safe, repurposed drugs). Personally, I obtained Sulodexide from abroad for a cost of ~$180 for a one month supply, and when I shared images of the package, medication blister packs and package insert with a Russian-reading pharmacist, he validated that I had the genuine article. Buyer beware, as I can’t speak for the ethics and quality control of the person on the other end of such transactions, and you would be purchasing the drug at your own risk.
P.S. Dr Pierre Kory and I are co-owners of The Leading Edge Clinic, a telemedicine practice. We work with a mission-focused staff of fifteen, including two extraordinary FNPs, India Scott and Laura Bevis. India and Laura also offer care in general medicine, and Laura specializes in geriatrics. We continue to study and learn in our treatment of PASC and vaccine injury. As one of five clinical sites participating in the five year FLCCC study using repurposed therapeutics as adjunctive treatment of cancer, Pierre and I are developing our expertise in this new realm. We will be joined full-time by another physician in August of 2024, who will focusing on cancer and which will significantly expand our capacity to help cancer patients. You can to go to our website at drpierrkory.com and initiate an application to become a patient in our practice.
My family moved from Horsham, PA to West Hartford, CT in 1973. For the next six years, we would make trips back to Pennsylvania for holidays such as Easter, occasionally Christmas, but always Thanksgiving. The Marsland clan holiday was Thanksgiving, and was spent in Parkerford with my Nana and Pop pop.
During the decade that my wife and I lived in Philadelphia, we made the trip to CT and back many times. The experience of a five and a half hour drive as an adult is soooooo different than that of a child. You have a steering wheel in your hands, your foot on the gas and brake pedals, and must pay attention. Driving is the most complex behavior which many of us engage in on a regular basis, judging distance and speed, calculating risk, and exercising situational awareness.
As a child in the backseat, five and a half hours was a prolonged period of boredom, counterbalanced by the adrenaline-filled anticipation of seeing my grandparents. My little sister Sharon would be seated in her car seat between me and my older brother John. Our occasional squabbles were limited by my mother’s sharp fingernails. There weren’t the tools of distraction which contemporary parents use, such as CD players extending from the ceiling or mounted on a headrest. The Sony Walkman hadn’t been invented yet. Thankfully, I was a reader, and could spend some time engrossed in a book. Still in elementary school, I made my way through The Kent Family Chronicles, which were adult novels of adventure and romance by American writer John Jakes.
I didn’t recognize landmarks, but my body knew when we were getting close to Parkerford because of the change in texture and pattern of the roads. There was a series of stop lights as we drove through Phoenixville and and past Spring City; some railroad tracks we would cross over, and then the left turn at the light off of Rt 724 onto Old Schuykill Rd. I knew that intersection, and felt the slower speed of the car for the next few minutes. My excitement grew until we turned left onto Zeiber Rd, reached the crest of the hill, and turned right into Nana and Pop pop’s gravel driveway.
Nana must have heard the crunch of tires on gravel, and would be at the door to greet us with a big wet kiss. She smelled like Dove soap. As I entered the tight space between the kitchen door and the basement door, I could smell a combination of cooking smells, with lingering elements of natural gas from the stove pilot light, cigar, and old wood. I swear that I could smell the Froot Loops among the little cereal boxes she would keep in the oven for our visits. (Why keep cereal in the oven, I will never know!) There was gentler, warmer lighting of incandescent bulbs, long before LEDs became pervasive. We would bring in our suitcases, and I would take a minute to bounce on the twin bed on my side of the room which I would share with my brother, listening for the reassuring squeak of the old box springs.
Pop pop would still be at the service station he ran in Norristown. I loved my Nana, but I adored my Pop pop. His return home was my highlight of our visits. He would be wearing his dark blue Dickie’s work shirt and pants with his black workshoes. He smelled like cigar and sweat with hints of gasoline and oil. He had a big smile of crooked tea-stained teeth, a rich laugh, and baritone timbre to his voice.
Before we could get down to playing a card game of Hearts or Oh Hell, or dominoes if it was later, Pop pop had to tally up the day’s receipts. He had an old Phillies cigar box, and I could smell the cash as he counted bills, doing long addition with a pencil and piece of paper. It was all so tangible and immediate.
As I drifted off to sleep, I could hear the tinkle of the old radiators, and in the middle of the night, my Pop pop’s snoring from the adjacent bedroom. Because of his work, he was an early riser both during his working years and in retirement. We kept our bedroom doors open, and even if I wasn’t ready to get out of bed yet, I could hear Pop pop’s footsteps on the hardwood floors as he passed our bedroom. I could smell the whiff of cigar smoke as he lit up before going outside for a walk. I didn’t need to ask “Are we there yet?” I was home.
RECENT PAST
Copenhagen Fall 1989
In the Fall of 1989 I was attending Denmark’s International Study program (DIS) in Copenhagen, Denmark. I was a Business Economics major back at Susquehanna University, a small liberal arts college in Central Pennsylvania, and was enrolled to study international business at DIS for my entire junior year. When Winter break came, I flew to Madrid, Spain to meet up with my friend Kelly Hayner, a former Susquehanna graduate who was now teaching English. It was a great visit, with late-night dancing, standing meals at tapas bars, and several day excursions. We paid a visit to Museo Reina Sofía, where Picasso’s Guernica and all of the steps leading up to its creation are displayed. We also traveled to Segovia to see the Roman aqueduct and its Gothic cathedral.
At the end of our visit, I boarded a plane in Madrid, with plans to land in Paris. When I was a teenager, I was an informal exchange student with la famille Tardiveau near Nantes, and intended to visit them again. The weather goddess had other plans, and, less than an hour after takeoff, our plane was diverted back to Madrid, where we were placed on a train instead. It was chaotic; babies were crying, kids were whining, and tempers were short.
There are more pigs than people in Denmark, and few people outside of Denmark would bother learning Danish, because most Danes speak excellent English, and German, and French. I noted that when Danes are traveling abroad, they are comfortable expressing themselves without restraint in their mother tongue, as they can rightly expect that no one else will know what the hell they are saying. I enjoy languages, and as usual was motivated by romance and lust, so took up studying Danish during my first semester at DIS.
Back to the train. I knew that the passengers were getting to the end of their patience, when I heard a deep man’s voice yell “Hold kæft!”, which is a crude way of saying shut up in Danish, in response to another passenger’s crying baby. Thankfully, the train arrived at the Gare Montparnasse within the hour. Unfortunately, it was now past midnight, and no trains were running again until 6:30am.
Gare Montparnasse
Being a college student with limited funds, I figured that I would just find a corner and doze against my backpack until later that morning. Two members of the Police Nationale and a nasty German Shepherd had other ideas, and sent me packing. They did give me space to stow my backpack in a locker, but a few minutes later I was standing outside the station getting the once-over by several prostitutes. I proceeded to walk across the street to enter an open cafe, thinking that I would hang out there for a while. I ordered an omelet with jus d’orange and half a baguette. I was about to order coffee when the waiter let me know they were closing. It was only 1:30am! I paid my bill and walked outside. It must have been a slow night, because the same prostitutes were giving me looks of reconsideration.
I flagged a taxi, and in my adequate French explained that I was looking for a restaurant that was open all night. He obliged me, and dropped me off on a street corner which had an open restaurant on each side. I walked up to the door which was closest to me, and as soon as I entered, felt out of place. Everyone looked like they had just come from the opera, wearing tuxedos and full-length dresses. I was wearing a red Marmot shell over a flannel shirt with blue jeans and hiking boots. The maître d’, without hesitation escorted me to a two-top with a fine linen tablecloth. The equally professional waiter arrived but a moment later to deliver a menu.
Everything on the menu looked good—and expensive! I picked the least expensive item I could find, which was a broiled white fish, which came with cream sauce, blanched asparagus, and a delectable whipped potato creation. I drank from une carafe d’eau, not daring to get into the wine list. I ate v-e-r-y s-l-o-w-l-y, but still, when I finished, it was only 3:00am. I paid my bill, walked out of the restaurant, and across the street to the other restaurant!
I’m not sure how to describe this third restaurant. It was brightly lit, and bustling with customers. The menu was eclectic, and I was not starving for sure, so I decided on a chef salad. When the salad arrived, it was huge! There were FOUR hard-boiled eggs, sliced in half, a generous amount of sliced ham and cheese, tomatoes, different types of lettuce, red onions, olives, and a lovely vinaigrette. I dug in, and even had some buttered baguette on the side. When I finished, it was…4:30 am.
I left the restaurant, thinking that I would get a cab, but when I counted up my remaining Francs, I realized that I had just enough money left to buy a train ticket. Well, then I could use the Metro. Wrong. The Metro stops were shuttered by iron gates. I didn’t have a map, but had been here three years before, and using the maps in the bus shelters I began to make my way back across the city to Gare Montparnasse. It was surreal. There was hardly anyone out and about, just a rare taxi and no other pedestrians. I walked by the Obelisk on Place de la Concorde, Jardin des Tuileries, the Louvre and its pyramid, all dramatic light and shadow in their spotlights. At first I was scared, but then just accepted my fate and enjoyed myself.
Obelisk at Place de Concorde
I arrived back at the Gare Montparnasse around 5:30 am, and it was starting to come to life. I got in line to buy a ticket to Nantes on a train leaving at 6:30am. In my well-structured but poorly pronounced French, I told the ticket counter clerk, “Je voudrais un billet pour le prochain train pour Nantes.” I.e. I would like a ticket for the next train to Nantes. The price of the ticket was unexpectedly low. I puzzled over this as I walked away, and as the minutes ticked by I came to understand my mistake. The clerk had heard my prochain (next) as chien (dog), and issued me a ticket for a dog!
It was now 6:00 am, and the ticket line was long. When I reached the clerk, again, I summoned up some indignity. (If you’ve ever heard an indignant Frenchman saying “Incroyable!”, you’ll understand). With pained emphasis and pronunciation, I said, “Je suis pas un chien (I’m not a dog), je suis un humain, et je voudrais, un billet, pour le prochain train pour Nantes!” Ah, this time he understood: with a quick grimace, he accepted my old ticket and issued a new one.
I got to the train about five minutes before departure. It had been more than twenty four hours, one train ride, two Police Nationales and one German Shepherd, two prostitutes, one taxi drive, three restaurants, three excellent meals, one very long and lovely walk, and one train station clerk, but I was finally on my train. I was already dreaming of the cozy bed awaiting me chez Tardiveau.
Toute la famille Tardiveau, juin 1986
PRESENT
Several times this week during patient visits, I fielded some form of the question: “When can I stop taking ______ prescription medication?” I usually respond with a question to try and gauge the patient’s willingness to continue—indefinitely. “What are your concerns about continuing with ______ medication?
Given that we are talking about post-acute sequelae of COVID (PASC) and vaccine injury, the relevant medications are most often IVM, LDN, Ketotifen, Eliquis, Plavix and Aspirin. But patients are also weary of taking fistfuls of supplements, and will ask about NAC Augmentata, Nattokinase, Lumbrokinase, etc.
When the patient’s primary concern is cost, I try to help them discern what the priorities of treatment are in each case, keeping in mind that there can be significant differences between patients. That is why I like the low-cost or free interventions such as intermittent fasting, extended fasting, grounding, prayer, meditation, cold-water showers, Baobab, Lithium, and alkaline water.
More often, patients just don’t want to keep taking a prescription drug. In part, it’s a self-image issue. Most patients with PASC and vaccine injury were high-performers in their lives before COVID. Their self-perception didn’t include having a pill organizer the size of a laptop with color-coding, nor did they expect that their Saturday night routine would include filling said pill organizer. Bless her soul, my wife got me some super-thoughtful Christmas presents last year, and not that a pill organizer wasn’t thoughtful, but damn, that wasn’t on my wish list for Santa.
I don’t have a crystal ball and, certainly, the front-row seat I have had to this genocide in progress has colored my perspective. Yup, I used the g-word, and mean every syllable of it. I expect patients (and you, dear reader) to take what I say with a boulder of Pink Himalayan sea salt. Yet I have a perspective that I think is worth sharing, otherwise I wouldn’t be spending some of my few free hours writing this.
Spikopathy is instigating a list of pathologies longer than…Fauci-Pinocchio’s nose during a recent congressional hearing. The world is contaminated with spike. Our bodies are contaminated with spike. I don’t know when or if that will ever end. Spike is provoking microclots, in all of us. Microclots provide refuge and mobility to metastatic cancer cells. Turbo cancer is a real thing, and in case nobody close to you has been diagnosed with cancer in the last two minutes, I’ll say that it arrives in the middle of the night and doesn’t wait to kiss you goodbye in the morning.
IVM blocks the influence of spike on platelets and red blood cells (RBCs), so that they are less inclined to aggregate and activate into microclots. LDN decreases the cytokine IL-6, a provocateur of mast cell activation, clotting, and cancer. Ketotifen stabilizes the mast cells which can be connected to every symptom a person has, from head to toe and everything in between. Because mast cells survive two to four years in our body, attending to their misbehaving ways is a priority. Eliquis, Plavix, Aspirin, Nattokinase, and Lumbrokinase are all helping our bodies cope with the burden of microclotting. NAC Augmentata breaks the disulfide bond between spike and ACE2 receptors, smashing spike into nearly 100 fragments so that our liver can break it down further and we can pee it out of our bodies. Every one of these therapies is doing something very important.
The comparative mind is a source of tremendous human suffering. “I look around and see everybody else living their lives, doing what they please, and they aren’t taking these drugs or supplements, they aren’t fasting, they’re not paying to speak with you every month. So, I ask again, how long do I have to take these drugs?”
Well, I can be blunt. First, there weren’t any classes in school about how you heal people from an intentional bioweapon. This is an on-the-job living classroom situation and we’re learning as we go. Second, third and fourth: how long do you want to live? How well do you want to live? How much of your mind do you want to keep? If your answers are, a long time, as well as possible, and all of it, then I would advise you, don’t stop taking those pills and potions.
Over the last thirty years, it has been my tremendous honor to be present as countless fellow humans grappled with their mortality, and often, while they passed over to the other side. For every person whose chronic illness has engendered bitterness in their soul, there is another who has made lemonade out of lemons, asked themselves what lessons they are meant to be learning, and made significant changes to how they live, in order to keep living. Sometimes these are people who are near death, but they are extracting meaning from their journey. By the calculus of Holocaust survivor Elie Wiesel: pain without meaning equals suffering.
Many of you had your eyes and ears open long before the lies and coercion to be vaccinated came tumbling down from on high. I was slower to pick up the plot, but I’ve been busy catching up. The last people I would be watching for clues about what to do next are the people who are doing nothing. I mean the people who are living their lives without a care, because they didn’t get a bad batch shot, and, by golly, those boosters were no trouble either! The time for wishful thinking is long gone. Never before in the history of humanity has our capacity to look squarely at reality been so important to our survival.
P.S. My colleague Dr Mobeen Syed or Dr Been has returned his focus to his medical education company, and recently completed a course on pain titled DEA Requirement for Opioid Use Disorder Management. For the medical professionals who read Lightning Bug: if you have suffered through tedious lectures which reinforce the pharma-influenced narrative in order to meet your obligatory CMEs, Dr Been’s lectures are a joy to behold. He is a brilliant and talented teacher, and you will learn concepts of anatomy, physiology, pharmacology, and practical treatment which will make your daily practice more interesting, and more effective. The cost is also very reasonable. For both practitioners and laypeople alike, I highly recommend the second lecture in this series, in order to understand the dynamics behind the chronic muscle pain which so many of us experience as a result of the spike protein.
P.S.S. I have no financial interest in Dr Been’s company.